Contributed by:
This content was developed by focusing on therapeutic responses by nurses to patients and families. Mental nursing is specialized nursing, hence a candidate is in much better shape if they focus on Therapeutic type of questions and Mental Health Pharmacology.
1.
Therapeutic Communication
Johncy Joseph RN-BSN, MBA
Avenir Solutions, LLC
2.
Useful Phrases
“Tell
“Are you me
saying…” about…
“Go on…”
”
“It seems as
if…” “What are
“What are you
your feeling…”
thoughts…”
3.
Forbidden Phrases
“Why don’t “It’s the policy
you…” on this unit…”
“You
should
…”
“Everyone “You’ll
…” have
“If it to…”
was me,
I’d…”
“You
“I
“Don’t can’t…”
worry…”
” “Just a
second…”
4.
Schizophrenia: Thought Disorder
Do not agree with or support delusions/hallucinations
Avoid arguing about delusions/hallucinations be very
matter-of-fact
Protect client from injury related to
delusions/hallucinations
Encourage any recognition of distorted reality
Discuss your observations with the client
5.
The nurse is conducting an initial assessment
interview with a newly admitted client whose
diagnosis is paranoid schizophrenic. When the
client says,” The voices are talking with me now.
They won’t go away, “ what is the most necessary
response of the nurse?
1. “I don’t hear the same sounds that you are
hearing.”
2. “Does what you’re hearing seem real to you?”
3. “Are you receiving a message from what you are
hearing?”
4. “What you’re hearing aren’t really voices of
people. They’re thoughts in your head.”
6.
A client with paranoid schizophrenia tells the nurse,
“I’m here on a secret mission for the government.
Don’t blow my cover.” Which response by the nurse
would be most therapeutic?
1. “Let’s talk about something other than your mission
for the government.”
2. “Your admission papers do not list you as a
government employee.”
3. “You have lost touch with reality, which is a
symptom of your illness.”
4. “It sounds like you have some concerns about your
privacy. You are safe here.”
7.
A client with the diagnosis of schizophrenia
watches the nurse pour juice for the morning
medication from an almost empty pitcher and
screams, “That juice is no good! It’s
poisoned.” The nurse should:
1. Remark, “You sound frightened.”
2. Assure the client that the juice is not
poisoned.
3. Pour the client a glass of juice from a full
pitcher.
4. Take a drink of the juice to show the client
that it is okay.
8.
The client who was admitted to the psychiatric unit 3
days ago is exhibiting increased restlessness and
hyperverbal speech and is wearing excessive make-up
and multi-colored clothes. The night shift staff has
reported that the client sleeps 2 hours per night. The
psychiatric nurse’s intervention will be:
1. Explain to the client the proper way to apply make-up.
2. Continue to monitor her sleeping patterns.
3. Discourage her from attending groups because her
behavior may be disruptive.
4. Discuss with the attending physician the need to
obtain a lithium level because the client may be
“cheeking” her lithium.
9.
A relative brings a client with schizophrenia to an outpatient unit
in a disheveled state. The client is inappropriately dressed and
inattentive to the staff due to visual and auditory hallucinations.
The client is started on haloperidol (Haldol). At the follow-up visit
to the clinic, which is the best indicator that the Haldol is having
the desired effect? The client:
A ) arrives independently at the clinic by bus one hour late for the
appointment.
B ) glances off into the corner of the room.
C ) takes a bath and wears clean, appropriate clothing with the
family's constant urging.
D ) walks restlessly when awake and sleeps almost twelve hours
every day.
10.
Depression: Mood Disorder
An important nursing intervention with the depressed client is
to sit quietly with them, offering support with your presence
Loss of ability to think clearly or concentrate.
They have difficulty hearing/accepting compliments so offer
acknowledgements on noted behavior improvements.
Suicidal-directly ask about intent, inform cannot remain
confidential, be wary of depressed patient who becomes
“better/happy”, stay with patient-never leave alone, offer
hope
11.
One day the nurse sits by a depressed client’s
bed and states, “I will be spending some time
with you today.” The client responds angrily,
“Go talk to someone else. They need you
more.” The most therapeutic response by the
nurse would be:
1. “Why are you angry with me?”
2. “I’ll go, but I will be back tomorrow.”
3. “Don’t say that. You are important, too.”
4. “I will be spending the next 15 minutes with
you.”
12.
A male client with the diagnosis of bipolar
disease disorder, depressed type, is found
lying on the floor in his room in the psychiatric
unit. He states, I don’t deserve a comfortable
bed; give it to someone else.” The nurse
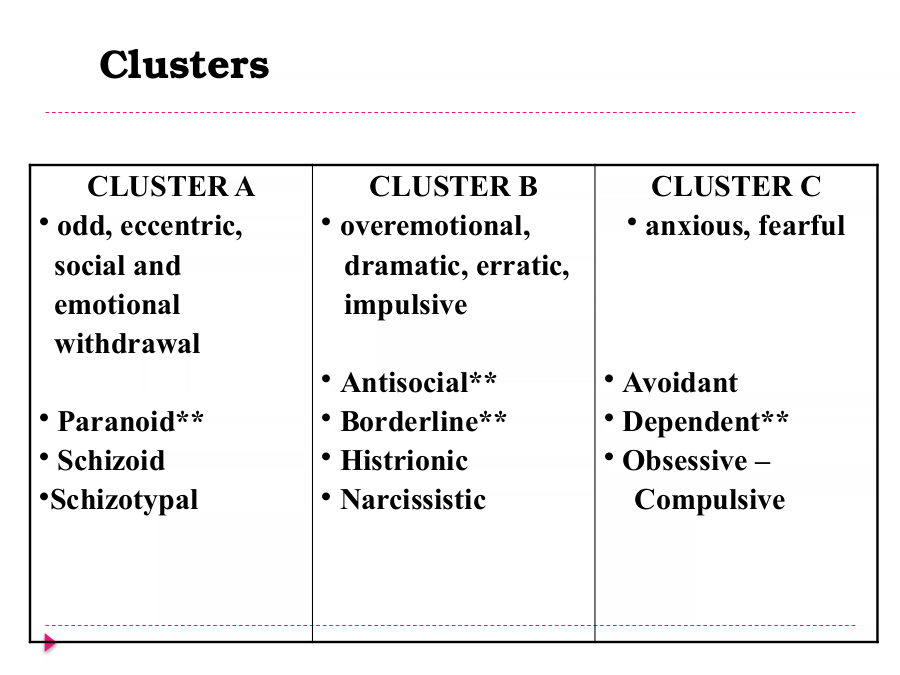
should respond:
1. “Everyone has a bed and this one is yours.”
2. “You are not allowed to sleep on the floor.”
3. “I don’t understand why you are on the
floor.”
4. “You’re too valuable a person to be lying on
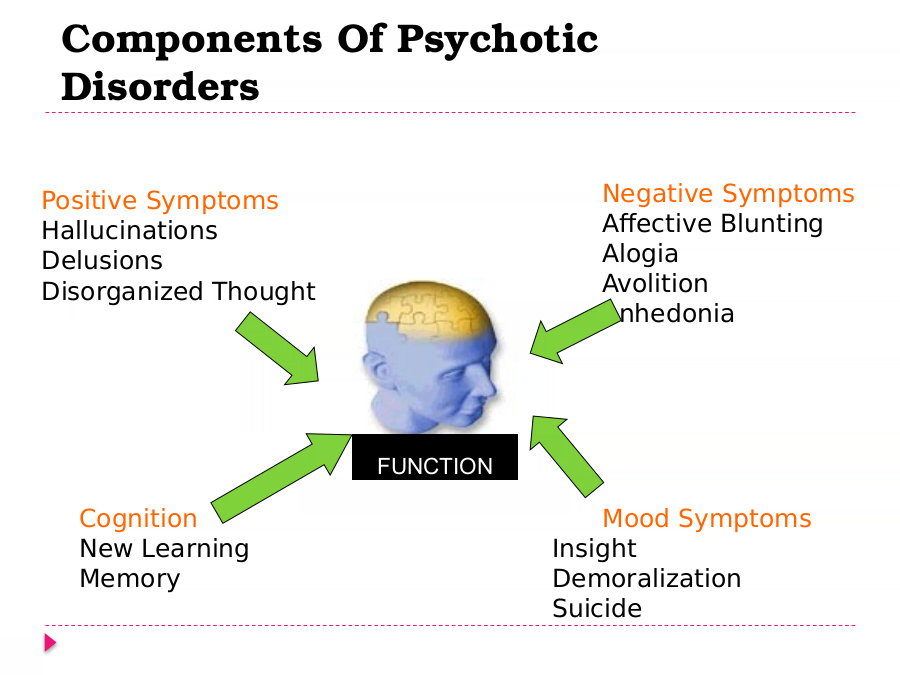
the floor.”
13.
As a young male client is receiving a dialysis treatment,
the nurse notes he is not talking with the other clients
and his eyes are lowered and his jaw is clenched. The
nurse states, “You look discouraged.” The client replies,
“I’m a bother. Not much good to anyone anymore. My
wife would at least get some insurance money if I died.”
The nurse’s most therapeutic response would be:
1. “I can understand how you feel.”
2. “You feel so bad you wish you were dead.”
3. “We all have days we feel like that. Let’s talk about your
diet.”
4. “I know it’s hard, but don’t let it get you down or let
your wife hear you.”
14.
Anurse states to a client, "Things will
look better tomorrow after a good
night's sleep." This is an example of
which communication technique?
A. The therapeutic technique of
"giving advice"
B. The therapeutic technique of
C. The nontherapeutic technique of
"presenting reality"
D. The nontherapeutic technique of
15.
Aclient diagnosed with post-traumatic
stress disorder is admitted to an inpatient
psychiatric unit for evaluation and
medication stabilization. Which
therapeutic communication technique
used by the nurse is an example of a
broad opening?
A. "What occurred prior to the rape, and
when did you go to the emergency
B. "What would you like to talk about?"
C. "I notice you seem uncomfortable
discussing this."
16.
Which therapeutic communication is the nursing
utilizing during a nurse-patient interaction?
Client: “When I get angry, I get into a fistfight
with my wife or I take it out on kids.”
Nurse: “I notice that you are smiling as you talk
about physical violence.”
A. Comparison
B. Exploring
C. Formulating a plan of action
D. Making Observations
17.
Afterassertiveness training, a formerly
passive client appropriately confronts a peer
in group therapy. The group leader states,
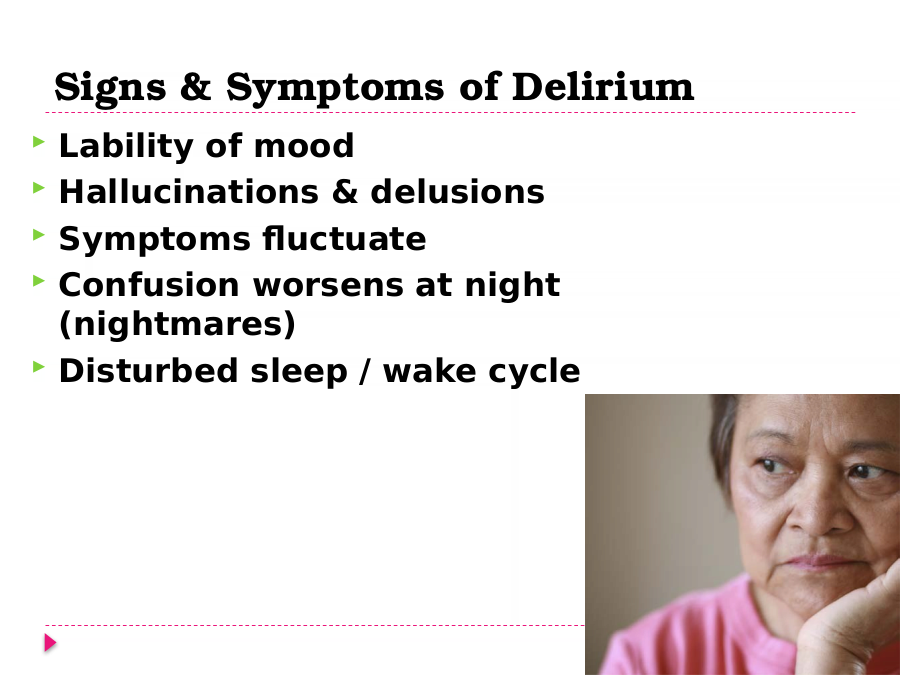
"I'm so proud of you for being assertive. You
are so good!" Which communication
technique has the leader employed?
A. The nontherapeutic technique of giving
approval
B. The nontherapeutic technique of
interpreting
C. The therapeutic technique of presenting
reality
D. The therapeutic technique of making
observations
18.
What is the purpose of a nurse providing
appropriate feedback?
A. To give the client good advice
B. To advise the client on appropriate
behaviors
C. To evaluate the client's behavior
D. To give the client critical information
19.
A client who frequently exhibits angry outbursts is
diagnosed with antisocial personality disorder.
Which appropriate feedback should a nurse provide
when this client experiences an angry outburst?
A. "Why do you continue to alienate your peers by
your angry outbursts?"
B. "You accomplish nothing when you lose your
temper like that."
C. "Showing your anger in that manner is very
childish and insensitive."
D. "During group, you raised your voice, yelled at a
peer, left, and slammed the door."
20.
A client diagnosed with dependant personality
disorder states, "Do you think I should move
from my parent's house and get a job?" Which
nursing response is most appropriate?
A. "It would be best to do that in order to
increase independence."
B. "Why would you want to leave a secure
home?"
C. "Let's discuss and explore all of your
options."
D. "I'm afraid you would feel very guilty
leaving your parents."
21.
A mother rescues two of her four children from a
house fire. In the emergency department, she cries,
"I should have gone back in to get them. I should
have died, not them." What is the nurse's best
response?
A. "The smoke was too thick. You couldn't have gone
back in."
B. "You're feeling guilty because you weren't able to
save your children."
C. "Focus on the fact that you could have lost all four
of your children."
D. "It's best if you try not to think about what
happened. Try to move on."
22.
A newly admitted client diagnosed with obsessive-
compulsive disorder (OCD) washes hands continually.
This behavior prevents unit activity attendance.
Which nursing statement best addresses this
situation?
A. "Everyone diagnosed with OCD needs to control
their ritualistic behaviors."
B. "It is important for you to discontinue these
ritualistic behaviors."
C. "Why are you asking for help if you won't
participate in unit therapy?"
D. "Let's figure out a way for you to attend unit
activities and still wash your hands."
23.
Which example of a therapeutic
communication technique would be effective
in the planning phase of the nursing process?
A. "We've discussed past coping skills. Let's
see if these coping skills can be effective
now."
B. "Please tell me in your own words what
brought you to the hospital."
C. "This new approach worked for you. Keep it
up."
D. "I notice that you seem to be responding to
voices that I do not hear."
24.
A client tells the nurse, "I feel bad because my
mother does not want me to return home
after I leave the hospital." Which nursing
response is therapeutic?
A. "It's quite common for clients to feel that
way after a lengthy hospitalization."
B. "Why don't you talk to your mother? You
may find out she doesn't feel that way."
C. "Your mother seems like an understanding
person. I'll help you approach her."
D. "You feel that your mother does not want
you to come back home?"
25.
A client's younger daughter is ignoring curfew.
The client states, "I'm afraid she will get
pregnant." The nurse responds, "Hang in
there. Don't you think she has a lot to learn
about life?" This is an example of which
communication block?
A. Requesting an explanation
B. Belittling the client
C. Making stereotyped comments
D. Probing
26.
When interviewing a client, which nonverbal
behavior should a nurse employ?
A. Maintaining indirect eye contact with the
client
B. Providing space by leaning back away from
the client
C. Sitting squarely, facing the client
D. Maintaining open posture with arms and
legs crossed
27.
Anurse is assessing a client diagnosed
with schizophrenia for the presence of
hallucinations. Which therapeutic
communication technique used by the
nurse is an example of making
A. "You appear to be talking to someone I
do not see."
B. "Please describe what you are seeing."
C. "Why do you continually look in the
corner of this room?"
D. "If you hum a tune, the voices may not
be so distracting."
28.
The nurse working with the family of a client with suicidal
ideations is asked if the medication the client is taking
will prevent suicide. Which of the following would be the
best response by the nurse?
1. “Clients who take their medication as prescribed are at
decreased risk for suicide.”
2. “Medication helps to treat an underlying mood disorder
associated with suicidal thinking and therefore prevents
suicide.”
3. “Medication can help decrease the frequency and
intensity of suicidal thoughts.”
4. “The client has said that she would never try to hurt
herself again. There is no need to worry.”
29.
Anurse maintains an uncrossed arm and
leg posture. This nonverbal behavior is
reflective of which letter of the SOLER
acronym for active listening?
A. S
B. O
C. L
D. E
E. R
30.
Identify the therapeutic communication technique
being used during a Nurse-patient interaction?
Client : “My father often disciplined me by spanking.”
Nurse: “Your father was a harsh disciplinarian.”
A. Restatement
B. Offering general leads
C. Focusing
D. Accepting
31.
An instructor is correcting a nursing student's
clinical worksheet. Which instructor statement is
the best example of effective feedback?
A. "Why did you use the client's name on your
clinical worksheet?"
B. "You were very careless to refer to your client by
name on your clinical worksheet."
C. "Surely you didn't do this deliberately, but you
breeched confidentiality by using the client's
name."
D. "It is disappointing that after being told, you're
still using client names on your worksheet."
32.
Which nursing statement is a good example of
the therapeutic communication technique of
giving recognition?
A. "You did not attend group today. Can we
talk about that?"
B. "I'll sit with you until it is time for your
family session."
C. "I notice you are wearing a new dress and
you have washed your hair."
D. "I'm happy that you are now taking your
medications. They will really help."
33.
A client is struggling to explore and solve a
problem. Which nursing statement would
verbalize the implication of the client's
actions?
A. "You seem to be motivated to change your
behavior."
B. "How will these changes affect your family
relationships?"
C. "Why don't you make a list of the behaviors
you need to change."
D. "The team recommends that you make only
one behavioral change at a time."
34.
The nurse asks a newly admitted client, "What
can we do to help you?" What is the purpose
of this therapeutic communication technique?
A. To reframe the client's thoughts about
mental health treatment
B. To put the client at ease
C. To explore a subject, idea, experience, or
relationship
D. To communicate that the nurse is listening
to the conversation
35.
A student nurse is learning about the appropriate use
of touch when communicating with clients diagnosed
with psychiatric disorders. Which statement by the
instructor best provides information about this aspect
of therapeutic communication?
A. "Touch carries a different meaning for different
individuals."
B. "Touch is often used when deescalating volatile
client situations."
C. "Touch is used to convey interest and warmth."
D. "Touch is best combined with empathy when
dealing with anxious clients."
36.
Which nursing statement is a good example of
the therapeutic communication technique of
focusing?
A. "Describe one of the best things that
happened to you this week."
B. "I'm having a difficult time understanding
what you mean."
C. "Your counseling session is in 30 minutes.
I'll stay with you until then."
D. "You mentioned your relationship with your
father. Let's discuss that further."
37.
After fasting from 10 p.m. the previous evening, a
client finds out that the blood test has been canceled.
The client swears at the nurse and states, "You are
incompetent!" Which is the nurse's best response?
A. "Do you believe that I was the cause of your blood
test being canceled?"
B. "I see that you are upset, but I feel uncomfortable
when you swear at me."
C. "Have you ever thought about ways to express
anger appropriately?"
D. "I'll give you some space. Let me know if you need
anything."
38.
During a nurse-client interaction, which
nursing statement may belittle the client's
feelings and concerns?
A. "Don't worry. Everything will be alright."
B. "You appear uptight."
C. "I notice you have bitten your nails to the
quick."
D. "You are jumping to conclusions."
39.
A client on an inpatient psychiatric unit tells
the nurse, "I should have died because I am
totally worthless." In order to encourage the
client to continue talking about feelings, which
should be the nurse's initial response?
A. "How would your family feel if you died?"
B. "You feel worthless now, but that can
change with time."
C. "You've been feeling sad and alone for
some time now?"
D. "It is great that you have come in for help."
40.
Which nursing response is an example of the
nontherapeutic communication block of
requesting an explanation?
A. "Can you tell me why you said that?"
B. "Keep your chin up. I'll explain the
procedure to you."
C. "There is always an explanation for both
good and bad behaviors."
D. "Are you not understanding the explanation
I provided?"
41.
A client states, "You won't believe what my
husband said to me during visiting hours. He
has no right treating me that way." Which
nursing response would best assess the
situation that occurred?
A. "Does your husband treat you like this very
often?"
B. "What do you think is your role in this
relationship?"
C. "Why do you think he behaved like that?"
D. "Describe what happened during your time
with your husband."
42.
Which therapeutic communication technique
should the nurse use when communicating
with a client who is experiencing auditory
hallucinations?
A. "My sister has the same diagnosis as you
and she also hears voices."
B. "I understand that the voices seem real to
you, but I do not hear any voices."
C. "Why not turn up the radio so that the
voices are muted."
D. "I wouldn't worry about these voices. The
medication will make them disappear."
43.
Which nursing statement is a good example of
the therapeutic communication technique of
offering self?
A. "I think it would be great if you talked about
that problem during our next group session."
B. "Would you like me to accompany you to
your electroconvulsive therapy treatment?"
C. "I notice that you are offering help to other
peers in the milieu."
D. "After discharge, would you like to meet me
for lunch to review your outpatient progress?"
44.
A client slammed a door on the unit several times. The
nurse responds, "You seem angry." The client states,
"I'm not angry." What therapeutic communication
technique has the nurse employed and what defense
mechanism is the client unconsciously demonstrating?
A. Making observations and the defense mechanism of
suppression
B. Verbalizing the implied and the defense mechanism
of denial
C. Reflection and the defense mechanism of projection
D. Encouraging descriptions of perceptions and the
defense mechanism of displacement
45.
Which of the following individuals are
communicating a non-verbal message? (Select
all that apply.)
A. A mother spanking her son for playing with
matches
B. A teenage boy isolating himself and playing
loud music
C. A biker sporting an eagle tattoo on his
biceps
D. A teenage girl writing, "No one understands
me"
E. A father checking for new e-mail on a
regular basis
46.
The nurse tells a client that talking with the staff
members is part of the therapy program. The client
responds, “I don’t see how talking to you can possibly
help.” The nurse’s most appropriate response would be:
1. “You will never know whether or not it is helpful unless
you are willing to give it a try.”
2. “I can see how you would feel that way now , but
hopefully you’ll change your mind.”
3. “The one-to-one relationship has proven itself very
helpful to others. Why don’t you give it a try?”
4. “Hopefully, I can help you sort out your thoughts and
feelings so you can better understand them.”
47.
A 40 year old client has a long history of
alcohol abuse. After an automobile accident
the client is arrested for driving while
intoxicated and is admitted to the hospital.
When the client becomes angry and blames
others, the nurse can be most therapeutic by
stating:
1. “You know you are to blame for your alcohol
abuse.”
2. “You need help now or you are going to get
sicker.”
3. “I can see that you are irritable and I want to
help you feel better.”
48.
Identify the therapeutic technique being used in the
nurse-patient interaction?
Client: “When I am anxious, I need alcohol to calm
down.”
Nurse: “Do you use any other alternatives to lower
anxiety?”
A. Reflection
B. Observation
C. Formulating plan of action
D. Giving recoginition
49.
The nurse is interviewing a newly admitted
psychiatric client. Which nursing statement
is an example of offering a "general lead"?
A. "Do you know why you are here?"
B. "Are you feeling depressed or anxious?"
C. "Yes, I see. Go on."
D. "Can you chronologically order the
events that led to your admission?"
50.
The client will be discharged to home tomorrow on an
antidepressant medication that will be taken once daily in the
morning . He asks, “Do I have to take the medication every
day?” How will I be able to sleep when I go home?” Do you
think I’ll be able to work, too, even though I have been in the
hospital this long? The nurse’s best response is:
1. “The best approach is to take it one step at a time, so that
everything will work out.”
2. “I understand you’re worried, but you and your wife will
decide tomorrow when you get home.”
3. “You seem to be worried about when you get home and how
you will function. Would you like to sit and discuss a plan for
your daily activities?”
4. “I’ll do my best to set up a plan for discharge that you can
take home with you and refer to later.”
51.
A 15 year old male is admitted to the adolescent unit
after attempting suicide. He verbalizes to the
psychiatric unit staff that he felt he was worthless, that
he couldn’t do anything right, and that no one would
care if he was gone. The psychiatric nurse demonstrates
therapeutic communication when she responds:
1. “I’m a mother and I know that I would be devastated if
my child committed suicide.”
2. “Do you realize that it’s a sin to commit suicide?”
3. “Tell me more about why you feel worthless and not
worthy of living?”
4. “I appreciate you trusting me with your feelings. I will
keep what you tell me just between us.”
52.
Doug, age 17, has come to the school nurse's office to talk
about his friend, Mike, also 17. Which statement by Doug would
indicate a need for immediate action by the nurse?
A ) Mike says his father hits him when he (the father) drinks.
B ) Mike has told Doug he wishes he could go to sleep and never
wake up.
C ) Mike plans suicide by driving his car off the road after school.
D ) Mike drinks beer on the weekends and is usually drunk each
night.
53.
Mr. Owen, age 78, has been admitted to the
psychiatric unit with a diagnosis of
Alzheimer's Disease. He says, “I really like this
hotel.” The most appropriate response for
the nurse is to say:
A ) Nothing
B ) “This is the hospital, Mr. Owen.”
C ) “Don't you remember where you are?”
D ) “It is nice, isn't it?”
54.
A client is brought to the alcohol detoxification unit
by his wife. He is lucid and cooperative with the
nurse during the initial interview. Which of these
questions is most important to ask during the first
interview?
A ) "When did you take you last drink?"
B ) "Do you usually drink at home or in a bar?"
C ) "Is it your decision to get help or is it your wife's
decision?"
D ) "Have you ever been to an AA meeting?"
55.
The spouse of a dying client says to the nurse, “ I don’t think I
can come anymore and watch her die. It’s chewing me up too
much!” The nurse should make which therapeutic response to
the spouse?
1. “Focus on your wife’s pain rather than yours. I know it’s hard,
but this isn’t about what’s happening to you, you know.”
2. “I know it’s hard for you, but she would know if you’re not
there, and you would feel so very guilty all of the rest of your
days.”
3. “It’s hard to watch someone you love to die. You’ve been here
with your wife every day. Are you taking any time for
yourself?”
4. “I think you’re making the right decision. Your wife knows you
love her. You don’t have to come every day. I’ll take care of
her.”
56.
A client who is suffering from urticaria (hives) and pruritis
says to the nurse, “What am I going to do? I’m getting
married next week, and I’ll probably be covered in this
rash and itching like crazy.” Which of the following
statements made by the nurse is the most therapeutic?
1. “You’re troubled that this will extend into your wedding?’
2. “It’s probably just due to pre-wedding jitters. You’ll be
fine.”
3. “The antihistamines will help a great deal, just wait and
see.”
4. “I hope your husband-to-be has a sense of humor and
can laugh about this.”
57.
A 23-year-old male client is admitted to a psychiatric
emergency unit after having been picked up by the police. He
was walking around a residential neighborhood at night
without shoes in the snow. The client appears confused and
disoriented. What nursing action is of highest priority?
a) Assess and stabilize his physical needs.
b) Assess and stabilize his psychosocial needs.
c) Arrange for transfer to a medical unit.
d) Attempt to contact a family member to obtain an accurate
history.
58.
When a nurse is assessing a client’s risk for
self-directed violence, which condition would
be the most significant?
a) Lethality of the plan
b) Degree if depression
c) A family history of suicide
d) Lack of a support system
59.
A 40-year-old homemaker presents to the triage area of
the ER with uncontrollable crying and anxiety. She states
her husband of 18 years has recently asked for a
divorce. The client is observed fidgeting in a chair and
wringing her hands. Which response by the nurse is
most therapeutic?
a) “You must stop crying so we can discuss your feelings
about the divorce.”
b) “Once you find a job, you will feel better and more
secure in your new life.”
c) “I can see how upset you are. Let’s sit here and talk
about how you’re feeling.”
d) “Once you have a lawyer looking out for your interests,
you will feel better.”
60.
Which of the following is most important in
planning care for a client experiencing sleep
deprivation?
a) Sleep is influenced by biological rhythms.
b) The natural body clock follows a 24-hour
cycle.
c) The longer a person sleeps, the more rapid-
eye-movement periods are experienced.
d) Prolonged periods of sleep deprivation can
lead to hallucinations and delusions.
61.
A male client is learning ways to better cope
with stress and anxiety. What is the primary
goal of this therapy?
a) The client will change his lifestyle.
b) The client will alter his response to stress.
c) The client will ignore situations that cause
stress.
d) The client will limit major sources of stress.
62.
The nurse is working with a client who appears to
be responding to voices. The client yells out at
intervals, “No, no I didn’t kill him. You know the
truth. Please help me!” The nurse should:
a) Sit quietly and not respond at all to the client’s
statements.
b) Respond to the client by asking, “Whom are they
saying you killed?”
c) Respond by saying, “I want to help you, and I
realize that you must be very scared.”
d) Say, “Don’t become so upset. No one is talking to
you. The accusing voices are part of your illness.”
63.
A nurse is performing an assessment on a 16
year old female client who has been
diagnosed with anorexia nervosa. Which
statement by the client would the nurse
identify as a priority requiring further
assessment?
1. “I check my weight every day without fail.”
2. “I exercise 3 to 4 hours every day to keep
my slim figure.”
3. “I’ve been told that I am 10% below my ideal
body weight.”
4. “My best friend was in the hospital with this
disorder a year ago.”
64.
Mental Health Nursing
65.
Therapeutic Communication
Calculated, deliberate, purposeful, and
focused
Goals:
To obtain information, correct
distortions
Develop trust, safety
Explore feelings, provide support
Display a sense of caring
This is one of the single most
important tools for the psychiatric
mental health nurse.
66.
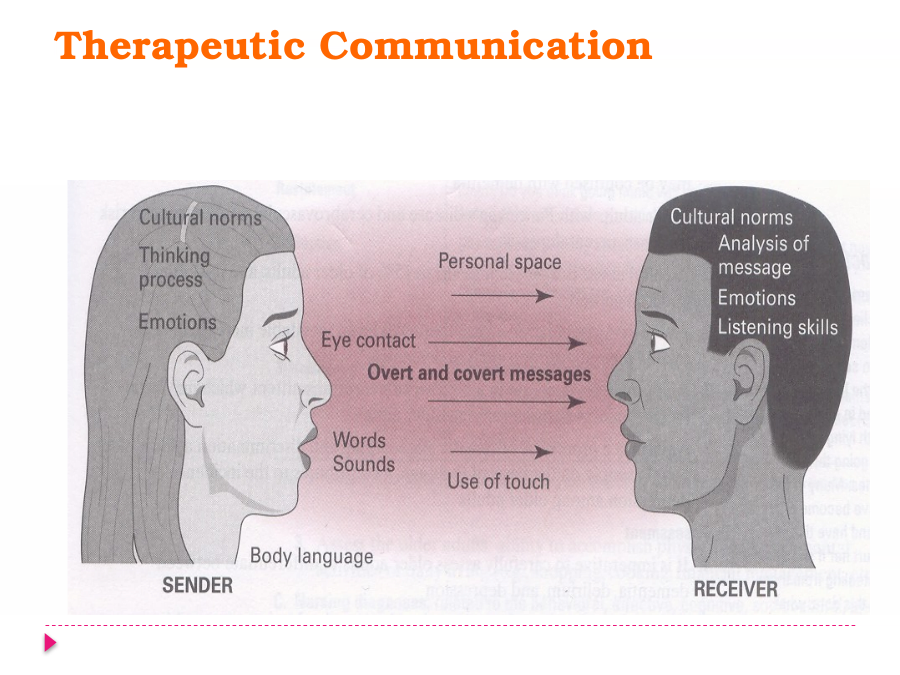
Therapeutic Communication
67.
Self Awareness
Use of self:
Know thyself, introspection: nurses know
more about themselves as they interact
with others, reflect on the interaction,
and are open to change.
Objectively examine: personal attitude,
beliefs,
motivations, strengths, limitations
Biases can impact interaction with
patients
Understand what motivated you to help
others:
patients do not take care of the nurses
emotional needs
68.
Different between Social and Professional
Social relationship Professional relationship
Interaction is primarily for Concerned with helping
reason of pleasure or the patients (regardless
companion-ship. their sex, religion, race…
etc.)
No person is in the Require the help of person
position of responsibility of with scientific knowledge
helping the other. and special skills (the
nurse).
There is no specific There is intention of
intention. dealing with other's
problem.
The goal is more or less The relationship is
social purposeful directed toward
a therapeutic goal.
It is up to the partners to The relationship should
share their personal affairs. not entail the nurse's
personal matters or
69.
Goals of Therapeutic
Communication
Establishing a therapeutic provider-client
relationship.
Identify client’s concerns and problem .
Assess client’s perception of the problem.
Recognize client’s needs.
Guide client towards a satisfying and
socially acceptable solution.
71.
Development of a Therapeutic Relationship
Boundary development and
maintenance:
Psychiatric patients often have an unclear
sense
of self (their responsibilities vs. others).
Every therapeutic relationship must have
clear
boundaries.
The RN must have a clear sense of
himself/herself and the role.
72.
Becoming a Better Listener
Concentrate on what is being said (content and
intent).
Observe facial expression and body language.
Respond by using your eyes, voice, gestures, and
posture to communicate empathy and
understanding.
Reflect the information you hear by paraphrasing
it.
Elicit more information-ask questions.
Control the desire to interrupt or pass judgment.
Take advantage of the lag time and notice the
speakers language and body gestures.
73.
Barriers to Communication
False reassurance
Closed questions
Giving advice
Defensive reflex
Making assumptions/ Value judgments
We hear what we expect to hear
Different perceptions
75.
Psychological and physiological status:
Gather information to complete patient
history
Physical exam: objective data
Laboratory and diagnostic tests
Psychological tests
76.
Phases of Therapeutic Nurse-Client Relationship
Pre-interaction Phase:
Before the initial contact
RN must reflect on personal biases, beliefs, values
• Orientation/Introductory Phase:
Acceptance, trust, and establish boundaries
Time frame and idenftiy expectations of the relationship
Proactively prepare the patient for relationship
termination due to limited time
77.
Phases of Therapeutic Nurse-Client Relationship
Working Phase:
Evaluate patient concern and problems
Let patient express their feelings and thoughts
Encourage patient independence for recovery
• Termination/Separation Phase
Evaluate progress and goal completion
Identify responses of relationship termination- anger,
sad, happy, dependency
Encourage client to express feelings
Identify patient’s strength and follow-up care
78.
Nurse must consider religious and spiritual
practices of the client and whether these practices
give the client hope, comfort, and support while
healing (Saunders, p1021)
Except in an emergency situation, client info cannot
be shared until specified by the client
Immediate nursing action for a client with anxiety is
to decrease stimuli in the environment and provide
a calm and quite environment
79.
Therapeutic Vs Non-Therapeutic
Therapeutic Non-Therapeutic
Clarifying and “Why” type questions
validating Defensive/Challenging
Encourage/Plan- Changing the subject
Give advice
based
Approval/disapproval
Patient
Stereotyping
focus/Listening
Judging/false assurance
Neutral
No encouragement
Responses/Silence
Acknowledge &
feedback
80.
Defense Mechanisms aka Coping
Compensation: Overachieve in one area to mask
failures- Example- Smoking compensated by
healthy eating
Conversion: Emotional disturbance become
physical symptoms Example- Post traumatic
disorder-paralysis
Denial- Failure to recognize circumstances –
Death of a loved one
Displacement: Feeling toward one person or
object due to someone else or thing- Arguing
with family due to work
Disassociation: Separation from conscious
81.
Defense Mechanisms aka Coping Mechanisms
Fixation: Never advancing to the next level of
maturation- Midlife crisis
Identification: Try to become someone else-
when people try to act like actors
Insulation/isolation- Being reserve- Depressed
patients
Intellectualization- Over reasoning to suppress
emotional conflict- Lovers
Introjection: Type of identification
Projection: Transferring one’s feelings towards
another- when an individual, threatened by his
own angry feelings, accuses another of hostile
thoughts.
82.
Defense Mechanisms aka Coping Mechanisms
Repression: Client blocks undesirable thoughts
from awareness
Resistance: Deep-seated opposition
Sublimation: replacement of unacceptable need
to a more social acceptable need- Men with
thoughts of infidelity will focus on fixing house/
women on diet draws pictures of food all the
time
Suppression: Forgetting of painful thoughts-
Childhood trauma
Symbolization: Use of an idea- Soldier defending
a flag
83.
Involuntary Admission
When a patient is ill or danger to self or others
Need of psychiatric treatment or physical care
Patient still retains
Right of informed consent
Right of refusal-unless court ordered/danger to self-other
Out patient treatment if possible
Require a court order- except in emergency/
legal counsel is mandated to the patient
Court hearing may be required for
discharge/commitment to a facility
Legally competent unless declared incompetent
through court
84.
Voluntary Release
Can be released voluntarily- AMA
If voluntary admitted- right to demand and
receive release
Unless danger to self or others- patient can be
released if voluntarily admitted
If voluntary admitted but dangerous- provider
can seek involuntary detention while court
proceedings declare the status of patient
Conditional release- Outpatient care, based on
compliance
Involuntary admission- if released can be
readmitted/re-institutionalized while seeking
court orders
85.
Models of Care/Types of Therapy
Milieu Therapy: Physical or social environment
patient receiving care
Safe environment- Safety is the priority
Community meetings, activity group, social skills
group, physical exercise groups
One to one relationship with staff
Encourage to express concerns, goals
Note- Goal of Milieu Therapy is to empower the
client through involvement in setting his or her
own goals and to develop therapeutic relationship
with staff to complete goals
86.
Models of Care/Types of Therapy
Interpersonal Psychotherapy: Therapeutic
Establish contract, clarify roles, work within a
time frame
Levels of Psychotherapy
Supportive Therapy
Allow the client to express and make decisions in a safe
environment- years
Re-educative Therapy
Learning new ways of thinking and behaving- longer
than support
Client enters in a contract that outlines desired
87.
Models of Therapy
Care/Types of Therapy
Active, directive, time-limited, and structured
approach
Based on patient’s attitude towards world
driven from past experiences
Psychoanalysis to identify the underlying
cause of distorted view of the world
Therapist focus on showing the patient how
irrational thought is harmful to the well being
of patient and others
Therapist help the patient change the way of
thinking to alleviate symptoms
88.
Models of Care/Types of Therapy
Group Therapy: Therapist and 5-8 clients within a
group but working on their own goals
Stages of Group Development
• Initial Stage: Acquaintances
Superficial relationship
• Working Stage:
Open and trusting communication
• Termination Stage
Begins at initial stage
Evaluation of goals, express concerns
89.
Group Therapy Models
Psychoanalytical Group Psychotherapy
Communication on 3 levels: conscious, semiconscious,
unconscious
• Transactional Analysis
Three ego states are analyzed
• Rogerian Therapy
Members express feelings towards each other in a non-
judgmental fashion
• Gestalt Therapy
Emphasis is on “here & now”- everyday problems
Self-expression/self-awareness/self-exploration
90.
Prominent Support Groups
Alcoholics Anonymous
Adult Children of Alcoholics
Cancer support groups
Gamblers Anonymous
Narcotics Anonymous
Parents without partners
Smoking Cessations groups
Mental Illness groups
91.
What Makes Your Psychological Health
ID: Personality from birth
Instinctual force behind your wants despite reality
Pleasure source
Freud- “ID is unconscious in nature”
Source of bodily needs
Wants
Desires
Impulses
Sexual Drives
Aggressive Drives
92.
What Makes Your Psychological Health?
EGO: Pleases ID desires while remaining in the
confines of reality- Makes you who you are- Your
Conscious awareness
Organizes thoughts- Develops with age & reality
Defensive, perceptual, intellectual-cognitive, and
executive functions (Planning, reasoning, memory)
Forms your morality, ethics, judgement
Individual’s safety- while satisfying needs of ID &
Superego
93.
What Makes Your Psychological Health
SUPEREGO: Consciousness based on social norms
taught by society (Parents, teachers, religion etc)
Aims for perfection
Enemy to ID
Acts in Socially appropriate manner
Controls the right or wrong in the context of social
norm
Symbolically- Father figure (Oedipus Complex)
94.
Somatoform Disorders
Individual complains or worry regarding
physical illness without supporting
physical findings
Symptoms increases with psychosocial
stressors
Client is fixated on signs and symptoms
Unable to control signs and symptoms
May be for increased attention and decrease
responsibilities
95.
Types of Somatoform Disorders
Conversion Disorders: Cause Unknown
Sudden onset of physical symptoms or deficit
Expression of psychological conflict or need
S/S- blindness, deafness, paralysis, mute
La belle indifference: Unconcerned with s/s
• Treatment
PT/OT/Speech Therapy
Stress Reduction Techniques
Cognitive Behavioral Therapy/Hypnosis
Anti-Depressants
96.
Types of Somatoform Disorders
Hypochondriasis: Obsession with the idea of
having a serious but undiagnosed medical
condition
long-term and intense fear
Counseling
Selective Serotonin Reuptake Inhibitor (SSRI)
Fluoxetine & Paroxetine
Pain Disorder: chronic pain experienced by a
patient in one or more areas due psycological
stress- Incapacitating
97.
Sleep Disorders
Sleep Disorders
Individual suffers from:
excessive daytime sleepiness
Inability to perform daily tasks safely and
properly
98.
Sleep Disorders
Dyssomnias: initiating or maintaining sleep or of
excessive sleepiness
Primary insomnia: trouble falling asleep or staying
asleep
Circadian sleep disorder: Unable to sleep at night
Breathing related sleep disorder: Sleep Apnea
Primary hypersomnia: excessive daytime sleepiness
Nightmare disorder: frequent nightmares- personal
safety
Sleep terror disorder: screaming, intense fear while
asleep
Sleepwalking disorder: Sleep walking and performing
task
100.
Anxiety and Mood Disorders
Anxiety Disorders:
characterized as anxiety and avoidant
behavior
feelings of impending doom, guilt,
shame
Mood Disorders:
Spectrum of moods ranging from
depression to mania
101.
Anxiety Disorders
Introduction
Anxiety provides the motivation for
achievement, a necessary force for survival.
Anxiety is often used interchangeably with
the word stress; however, they are not the
same.
Anxiety may be differentiated from fear in
that the former is an emotional process,
whereas fear is cognitive.
102.
Anxiety Disorders
Epidemiological statistics
Anxiety disorders most common type of all
psychiatric illnesses
More common in women than men
Also occurs in children
More prevalent in girls than in boys
Children in lower socioeconomic environments at
greatest risk
103.
Anxiety Disorders
How much is too much?
May be considered abnormal if
Anxiety is out of proportion to the
situation that is creating it
Anxiety interferes with social,
occupational, or other important
areas of functioning
104.
Anxiety Disorders
Panic disorder: assessment
Characterized by recurrent panic attacks,
onset of which are unpredictable, and
manifested by intense apprehension, fear,
or terror, often associated with feelings of
impending doom and accompanied by
intense physical discomfort
105.
Panic Disorder
Generalized anxiety disorder
Panic anxiety related to real or
perceived threat to biological integrity
or self-concept
Powerlessness related to impaired
cognition
Assessment
Characterized
by chronic,
unrealistic, and excessive
anxiety
and worry
106.
Panic Disorder
The client
Is able to recognize signs of
escalating anxiety
Is able to intervene so that anxiety does not
reach level of panic
Is able to discuss long-term plan to prevent
panic anxiety when stressful situations occur
Practices techniques of relaxation daily
Engages in physical exercise three times a
week
Performs activities of daily living
independently
Expresses satisfaction with independent
functioning
Is able to maintain anxiety at a manageable
level without use of medication
107.
Phobias
Agoraphobia without history of panic
disorder: Assessment
Fear of being in places or
situations from which escape
might be difficult or in which
help might not be available if a
limited-symptom attack or
panic-like symptoms
should occur
108.
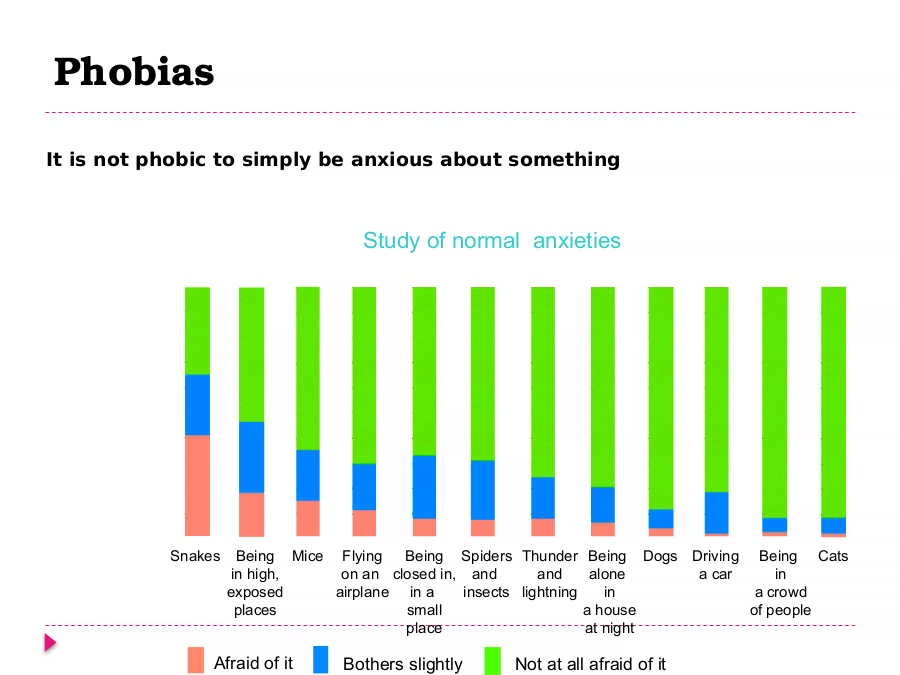
Phobias
It is not phobic to simply be anxious about something
Study of normal anxieties
100
Percentage 90
of people 80
surveyed 70
60
50
40
30
20
10
0
Snakes Being Mice Flying Being Spiders Thunder Being Dogs Driving Being Cats
in high, on an closed in, and and alone a car in
exposed airplane in a insects lightning in a crowd
places small a house of people
place at night
Afraid of it Bothers slightly Not at all afraid of it
109.
Social Phobias
• Fear of failing/being embarrassed
in public
– public speaking (stage fright)
– fear of crowds, strangers
– meeting new people
– eating in public
• Fears interfere with normal
behavior
• Equally often in males and females
110.
Phobias
Specific phobia: Assessment
Marked, persistent, and excessive or
unreasonable fear when in the presence of, or
when anticipating, an encounter with a specific
object or situation
Life experiences
Early experiences may set the stage
for phobic reactions later in life
111.
Phobias
The client
Functions adaptively in the presence
of the phobic object or situation without
experiencing panic anxiety
Discusses feelings that may have contributed
to irrational fears
Verbalizes a future plan of action for
responding in the presence of the phobic
object or situation to avoid developing panic
anxiety
Demonstrates techniques that can be used to
maintain anxiety at a manageable level
Voluntarily attends group activities and
interacts with peers
112.
Acrophobia: Height
Agoraphobia: Open Spaces Types of Phobias
Astraphobia: Electrical Storms
Claustrophobia: Closed spaces
Hematophobia: Blood
Hydrophobia: Water
Monophobia: Being alone
Mysophobia: Dirt or germs
Nyctophobia: Darkness
Pyrophobia: Fire
Social Phobia: Situations/embarrassed
Xenophobia: Strangers
Zoophobia: Animals
113.
Obsessive-Compulsive Disorder (OCD)
Assessment data
Recurrent
obsessions or
compulsions that
are severe enough
to be time-
consuming or to
cause marked
distress or
significant
impairment
114.
Obsessive-Compulsive Disorder (OCD)
Obsessions: Unwanted,
intrusive, persistent ideas,
thoughts, impulses, or images
that cause marked anxiety or
distress
115.
Obsessive-Compulsive Disorder (OCD)
Compulsions: Unwanted
repetitive behavior
patterns or mental acts
that are intended to
reduce anxiety, not to
provide pleasure or
gratification
116.
Obsessive-Compulsive Disorder (OCD) (cont.)
Diagnosis: outcome
identification
Ineffective coping
related to
underdeveloped ego,
punitive superego;
avoidance learning,
possible biochemical
changes
117.
Obsessive-Compulsive Disorder (OCD) (cont.)
The client
Is able to maintain anxiety at a manageable
level without resorting to the use of ritualistic
behavior
Is able to perform activities of daily living
independently
Verbalizes understanding of relationship
between anxiety and ritualistic behavior
Verbalizes specific situations that
in the past have provoked anxiety
and resulted in seeking relief
through rituals
118.
Obsessive-Compulsive Disorder (OCD)
Outcomes (cont.)
The client
Demonstrates more adaptive coping
strategies to deal with stress, such as
thought stopping, relaxation techniques,
and physical exercise
Is able to resume role-related
responsibilities because of decreased need
for ritualistic behaviors
Ineffective role performance related to
need to perform rituals evidenced by
inability to fulfill usual patterns of
responsibility
119.
Post-Traumatic Stress Disorder
Assessment
Development of
characteristic symptoms
following exposure to an
extreme traumatic stressor
involving a personal threat
to physical integrity or to the
physical integrity of others
For example: rape, child
abuse
120.
Post-Traumatic Stress Disorder
Characteristic symptoms
include re-experiencing the
traumatic event, a sustained
high level of anxiety or
arousal, or a general
numbing of responsiveness.
Intrusive recollections or
nightmares of the event
are common.
121.
Client/Family Education (cont.)
Management of the illness
Medication management
Possibleadverse effect
Length of time to take effect
What to expect from the medication
Stress management
Teach ways to interrupt escalating
anxiety.
Teach relaxation techniques.
122.
Client/Family Education (cont.)
Support services
Crisis hotline
Support groups
Individual psychotherapy
Treatment Modalities
Individual psychotherapy
Cognitive therapy
Behavior therapy
Systematic desensitization
Implosion therapy
Group/family therapy
123.
Treatment Modalities (cont.)
Psychopharmacology
Panic and generalized anxiety disorder
Anxiolytics
Antidepressants
Antihypertensive agents
Phobic disorders
Anxiolytics
Antidepressants
Antihypertensive agents
OCD
Antidepressants
124.
Treatment Modalities (cont.)
Psychopharmacology (cont.)
PTSD
Antidepressants
Anxiolytics
Antihypertensives
Others
126.
Mood Disorders
Spectrum of moods ranging from
depression to mania
Depression only = disorder
5 – 10% of U.S. adults suffer unipolar
depression in a given year
Essential assessment questions? unipolar
mood disorder
Depression + mania = bipolar
127.
Mood Disorder
Diagnostic issues
A number of “specifiers” (e.g.,
severity, chronicity) are used in
diagnosis
Two broad categories – unipolar and
bipolar
Two important criteria in diagnosis –
duration and severity
128.
Women and Depression
Women twice as likely as men
Higher rates of victimization
(child abuse, rape, battery)
Higher rates of poverty &
helplessness
Internalization vs.
Externalization
129.
Consider This
Euthymia: normal , positive
mood.
Hyperthymia: extremely happy
mood
Dyhthymia: Depressed mood
Cyclothymia: Mood swings
Dysphoria:
dissatisfaction/unhappiness may
cause depression, anxiety or
130.
Questions about Suicide Assessment
1. How should clinicians use knowledge
of suicide risk factors in their
assessment of patients at risk?
2. Which diagnoses, risk factors and
symptoms should most concern clinicians?
3. Is it ever acceptable to defer or avoid
hospitalizing a suicidal patient?
4. Should we expect antidepressants or
mood stabilizers to lower suicide risk?
5. What are the most important elements to
document in a suicide risk assessment?
131.
Bipolar I
Pure manic (unipolar mania)
or mixed episodes
132.
Lithium
Indications: Bipolar I (Manic epi.)/ Schizophrenia
Therapeutic Range: 0.5-1.5 mmol/L
Toxicity S/S: N-V-D, Dizziness, Stomach pains,
Generalized weakness
Nursing Consideration:
Hyponatremia can cause Lithium toxicity (Lasix)
133.
Bipolar II
Involves major depressive episodes (sadness or
hopelessness) and hypomanic episodes (irritable
or slightly elevated mood)
136.
Therapies for Mood Disorders
Beck’s cognitive-behavioral approach
involves changing thought patterns and
activity levels
Beck’s approach is an effective therapy for
depression
Social skills training involves improving
social interactions so as to lift
depression
137.
Biological Therapies for Mood Disorders
Electroconvulsive therapy (ECT) involves
the induction of brain seizures by the
application of electrical current to the
skull
ECT is an effective therapy for severe
depression, but its mechanism of action is
unknown
Drug therapy involves ingestion of
tricyclic drugs, MAO inhibitor drugs and
selective serotonin reuptake inhibitor
drugs
138.
Treatment for bipolar disorder
Popular Medications patients
Mood stabilizers:
Lithium
Depakote Psychoanalysis
Tegretol
There is no cure for
Anti-Depressants: bipolar disorder –
Wellbutrin
Prozac
it must be treated
Zoloft over a lifetime
Paxil
Haldol
Trilafon
Thorazine
Mellaril
Clozapine
Benzodiazepines (for anxiety &
Valium
Xanax
139.
Personality Disorders
140.
Personality Traits
Personality is a
consistent way of
thinking and feeling
which results from the
interaction of a
person’s genetic
make-up his level of
education and past
experiences.
Largely unconscious
Cannot be changed
easily
141.
Personality Disorders
Occur when traits become inflexible and
maladaptive but stable over time.
Cause either significant functional
impairment or subjective distress.
However they stay in the main stream
of society.
Present with symptoms more subtle
than other disorders.
142.
Clusters
CLUSTER A CLUSTER B CLUSTER C
• odd, eccentric, • overemotional, • anxious, fearful
social and dramatic, erratic,
emotional impulsive
withdrawal
• Antisocial** • Avoidant
• Paranoid** • Borderline** • Dependent**
• Schizoid • Histrionic • Obsessive –
•Schizotypal • Narcissistic Compulsive
143.
Personality Disorders
Antisocial: Total disregard
for the rights of others
BPD: Destructive,
impulsive, self mutilation,
emotional instability,
Dependent: Clinging, need
to have someone take care
of them
144.
Personality Disorders
Cluster A – Odd and Eccentric
• Paranoid – suspicious, argumentative (no
delusions or hallucinations)
• Schizoid – withdrawn, reserved, reclusive
• Schizotypal – eccentricity of thought and
behavior
145.
Personality Disorders
Cluster B – Dramatic, emotional, erratic
Antisocial personality disorder (APD)
• Defining feature is pervasive disregard for and
violation of rights of others
• Begins in childhood
• Must meet 3 of the following criteria – violation of
rights of others, nonconformity, callousness,
deceitfulness, irresponsibility, impulsivity,
aggressiveness, recklessness
147.
Defining Psychotic Behavior
Three Main Types
Perceptual Disturbances
Disorganized Thinking
Bizarre Beliefs
148.
Components Of Psychotic
Disorders
Positive Symptoms Negative Symptoms
Hallucinations Affective Blunting
Delusions Alogia
Disorganized Thought Avolition
Anhedonia
FUNCTION
Cognition Mood Symptoms
New Learning Insight
Memory Demoralization
Suicide
149.
Positive Symptoms - behaviors that are
present that should be absent:
Delusions, hallucinations, thought
disorders
Negative Symptoms - behaviors
that are absent that should be
present ;
Weak social interactions,
emotional expression, speech, and
working memory
150.
Schizophrenia
Catatonic: motionless despite external stimuli
Psychomotor characteristics
Disorganized
Disorganized speech and behavior,
incoherent thoughts, inappropriate or flat
affect
Paranoid
Easily angered, high risk for violence
151.
Features of Schizophrenia
Positive symptoms = represent excess or
distortion of normal behavior
Delusions = disorder of thought content
and presence of strong beliefs that are
misrepresentations of reality
Grandiose = belief that one has
special importance
Persecutory = belief that one is
the subject of a master plot;
feeling of being mistreated
152.
Nihilistic = Life is meaningless- Rejecting all
religious and cultural beliefs/ No moral values
Religious = involves some religious
theme
Very common; not diagnostically
specific
Bizarre = belief in something that could
not be true based on the person’s
culture
153.
Positive symptoms
Hallucinations = perceptual disturbance
in which things are sensed, although
they are not actually present
Auditory
Most common type of hallucination
Visual
Second most common type of hallucination
Other senses (olfactory, tactile, gustatory)
154.
Positive symptoms
Disorganized speech = style of
talking involving incoherence and
lack of typical logical patterns
• Clang association = rhyming
words
• Neologism = made-up words or
phrases
• Word salad = words/speech with
no message
• Derailment = deviation in the
train of thought
155.
Features of Schizophrenia
Negative symptoms = deficits in normal
behavior
Flat affect = emotionless demeanor when
a reaction would be expected
Avolition = apathy or inability to initiate
or persist in important activities
Alogia = deficiency in amount or content
of speech
Anhedonia = inability to experience
pleasure
156.
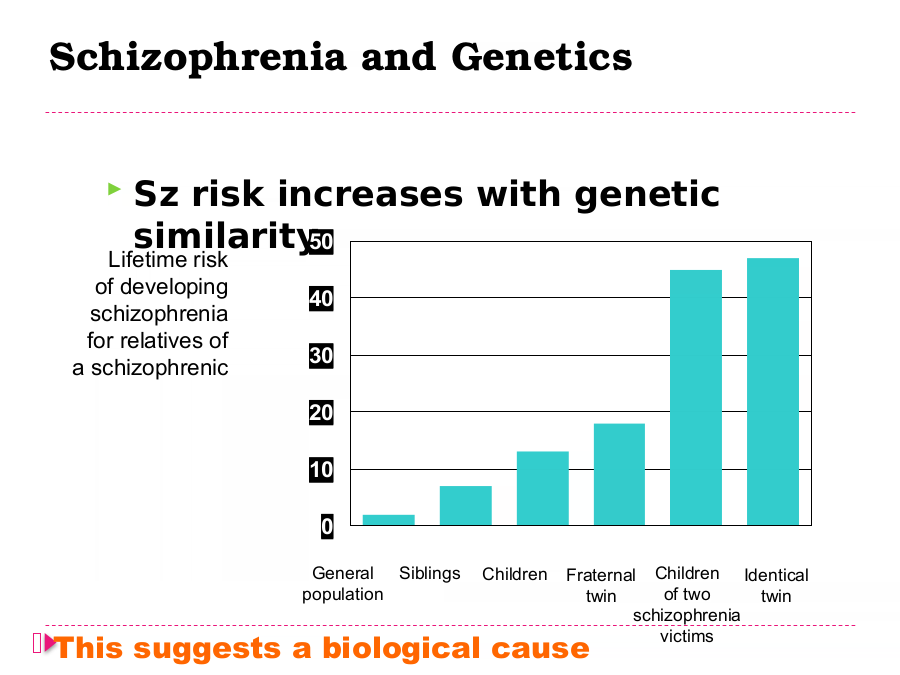
Schizophrenia and Genetics
Sz risk increases with genetic
similarity50
Lifetime risk
of developing
40 40
schizophrenia
for relatives of
30 30
a schizophrenic
20
20
10
10
0
0
General Siblings Children Fraternal Children Identical
population twin of two twin
schizophrenia
This suggests a biological cause victims
157.
Extrapyramidal Side Effects
Akathisia: Restlessness, fidgeting, pacing,
rocking , irritability
Dystonia: Torsions and spasms of muscle
groups
Pseudoparkinsonism:
Stiffness, shuffling, mask-like face, tremor,
rigidity
158.
Tardive Dyskinesia
Facial signs of TD: smacking, licking of lips,
chewing movements, rolling or protrusion of
tongue
Spastic facial distortions, ‘tics’
Jerking of fingers, ankles, toes, limbs, trunk,
neck, and pelvis
159.
Psychotherapeutic Management
Provide supportive care
Strengthen patient’s self-esteem
Treat patients as adults
Prevent failure/ embarrassment
Respect individuality - unique
Reinforce reality
Handle hostility calmly & matter-of-
factly
160.
Delusion & Nursing Intervention
Presenting reality, orient pts to time,
person & place
Avoid argument, touch, competitive
activities,
Reinforce positive behaviors
Encourage verbalization
161.
Disruptive Behavior
Set limit
Decrease environmental stimuli
Intervention before acting out
Close observation
Safety environment - minimize
potential weapons
Making contract with the client
Using restraints
162.
Withdrawn Patients
Arrange nonthreatening activities
Encourage participation - seating
Provide remotivation and resocialization
group experience
Reinforce appropriate grooming and
hygiene
Provide psychosocial rehabilitation -
social skill training, ...
163.
Nursing Interventions
Medication compliance- 40-60%
noncompliance
Avoid reinforcing hallucinations & delusion
Maintain orientation
Use touch minimally and judiciously
Avoid easily misinterpreted behavior
Reinforce positive behaviors
Avoid competitive activities,
Allow & encourage expression of feelings
164.
Second Generation Antipsychotics
Atypical
Clozapine (Clozaril)
Risperidone (Risperdal)
Olanzapine (Zyprexa)
Quetiapine (Seroquel)
Ziprasidone (Geodon)
165.
Substance Related Disorders
166.
Terms in Substance Use Disorders
Substance (drug) - affects body or
mind
Intoxication - temporary change
Abuse - excessive, chronic use &
impairment
Dependence - abuse + physical or
psychological dependence
tolerance
withdrawal
167.
Uppers (stimulants)
Cocaine (hydrochloride, “crack,”
freebase)
Amphetamines (“speed,” “meth,”
“ice”)
Amphetamine Congeners (Ritalin, diet
pills, e.g., fen/phen)
Plant stimulants (khat, betel nut, mate,
yohimbe)
Caffeine (coffee, tea, soft drinks, OTC
meds)
Nicotine (cigarettes, cigars, snuff,
168.
Increase central nervous system
Cocaine
euphoric rush of well-being,
confidence
increases dopamine in system
cocaine-induced psychosis
cheaper forms (free-basing, crack)
have increased abuse and dependence
problems
risk of overdose, suicide, heart
problems, brain seizures
169.
Downers (depressants)
Opiates/Opioids
(opium, codeine,
morphine, heroin, methadone,
Darvon, Percocet)
Sedative-Hypnotics
(benzodiazepines, e.g., Xanax,
Valium, Klonopin; barbiturates,
e.g., butalbital, Ambien, Miltown)
Ethyl Alcohol
Others (e.g., antihistamines,
170.
Slow activity of central nervous system
Alcohol
binds to GABA (inhibitory) receptors
intoxication associated with
decreased inhibition, slowed reaction
times, memory impairment
abuse can follow different patterns
(continual use, bingeing, etc.)
withdrawal
delirium tremens (DTs)
171.
Long-term effects of alcohol dependence
cirrhosis of the liver
lowers immune system
Korsakoff’s syndrome (confusion,
memory loss)
fetal alcohol syndrome (MR, slow
growth)
sedative-hypnotic drugs
barbituates
benzodiazepines
172.
opium
morphine
heroin
attach to receptors for endorphins
intoxication associated with pleasant,
calm feelings
withdrawal - anxiety, restlessness,
twitching, aches, fever
overdose - shuts down respiratory system
173.
All Arounders (psychedelics)
LSD, Psilocybin mushrooms, and
other indole psychedelics
Mescaline (peyote),
“ecstasy”(MDMA), & other
phenylaklylamine psychedelics
Belladonna, mandrake, & other
anticholinergic psychedelics
Ketamine, PCP, amanita mushrooms,
nutmeg, mace, kava
Marijuana & other cannabinoids
174.
Other drugs
Inhalants (organic solvents, volatile nitrites,
anesthetics)
Anabolic Steroids & other sports drugs.
Psychiatric Medications (antidepressants,
antipsychotics, antianxiety)
175.
Other substances
Cannabis
marijuana
hallucinogenic, depressant and
stimulant effects
more abuse and dependence now
than in 60s
memory impairment
lung disease
may interfere with human
reproduction
however, powerful anesthetic
176.
Alcohol Impairment
Blood Alc Level Consequences
0.02-0.05 Mildly impaired coordination
Potential changes in behavior
0.08-0.1 Impaired driving, slurred speech,
ataxia,
0.1-0.15 Impaired balance, gross judgment and
cognition
impairment
0.2-0.3 All sensory motor function impaired
0.3 & Potential cardiovascular and respiratory
collapse Coma, death
177.
CAGE Questionnaire
Screening Test for Alcohol
Dependence
C - Have you ever thought you should CUT
DOWN on your drinking?
A - Have you ever felt ANNOYED by others'
criticism of your drinking?
G - Have you ever felt GUILTY about your
drinking?
E - Do you have a morning EYE OPENER?
178.
EARLY 6-8 HOURS AFTER LAST DRINK
DT’S IN 72 HOURS
ANXIETY, ANOREXIA, INSOMNIA, N&V
TREMOR, “SHAKY”, DELIRIUM, ALTERED
L.O.C., PULSE & B.P., DIAPHORESIS
POSSIBLE SEIZURES
VISUAL, TACTILE HALLUCINATIONS
179.
Treatment Of Alcohol Withdrawal
Sedatives (Librium)
Thiamine
Magnesium Sulfate
Multivitamins
Antiemetics
--------------------------------------------------------
Antabuse Used during rehabilitation
phase only
180.
Psychodynamic
uncover underlying conflicts
Behavioral
aversion therapy
teaching alternative behaviors
contingency management
Cognitive-behavioral
Behavioral self-control training
Relapse Prevention
181.
Biological
detoxification
antagonist drugs
drug maintenance (methadone)
Socio-cultural
Alcoholics Anonymous
Residential Treatment programs
Community Prevention programs
182.
Dissociative Disorders
Depersonalization/Derealization: Outerbody
experience. Patient feels like a detached
observer
Dissociative Amnesia
Acute memory, consciousness, awareness,
identity, loss triggered by stress
Dissociative Identify Disorder
2 or more personalities in an individual
183.
Sexual Disorders
Gender Identity Disorder:
Individual wants to become/be like the
opposite
sex
Extremely uncomfortable with their
assigned gender role
Recurrent intense sexual urge/fantasy
Sexual Dysfunction
Disturbance in 1 or more phases of the
sexual response cycle
185.
Eating Disorders
Anorexia
deliberate
starvation may
engage in binge
eating & purging
186.
Anorexia Nervosa-Assessment
Less than 85% of Hypoglycemia
hypothermia
weight
Bradycardia, Lanugo, dry skin,
hypotension hair loss
Arrythmias Osteoporosis
Hypokalemia Constipation
187.
Anorexia Nervosa-Assessment
PHYSICAL SYMPTOMS
Less than 85% of normal weight
Bradycardia, hypotension
Arrythmias
Hypokalemia
Hypocalcemia
Dehydration
Amenorrhea
188.
Bulimia Nervosa
Recurrent episodes of uncontrolled
binge eating
Purging: a variety of compensatory
behaviors to rid self of food
Anxiety escalates before binging
Binges leads to feelings of loss of
control, guilt, depression,
humiliation and self loathing
Over-concern with body shape and
weight
189.
Bulimia Nervosa-Assessment
SYMPTOMS
Secretive eating
Frequency of binge varies
Abuse of laxative and diuretics
Close to normal weight maintained
190.
Bulimia Nervosa-Assessment
PHYSICAL SYMPTOMS
Bradycardia, hypotension,
arrythmias
Hypokalemia, hyponatremia,
dehydration
Irregular menses, hypogkacemia
Hoarseness,dental caries, enlarged
parotid glands, esophagitis
Constipation
191.
Major Cognitive Disorders
Alzheimers Type Dementia
Amnestic Disorders
Delirium
Vascular Dementia
192.
Cognitive Disorders
Any condition that alters or destroys
brain tissue
Symptoms include:
cognitive impairment
behavioral dysfunction
personality changes
193.
Cognitive Disorders Result from….
A primary brain disease
The brains response to a systemic
disturbance (medical condition)
The brains tissues reaction to a toxic
substance (D/A)
195.
Dementia
The word “Dementia” is used widely to describe a
group of diseases which affects the brain and
cause a progressive decline in a person’s abilities
to remember, think and learn. The main abilities
affected are:
Judgement
Orientation
Emotions
Memory
Thinking
196.
How Common Is Dementia?
Most older people do not get dementia.
It is not a normal part of ageing.
Dementia can happen to anyone at any
age, but becomes increasingly common
after the age of 65 years.
197.
Who Gets Dementia?
Approximately 1% of people over 75
years of age have dementia and the risk
of developing dementia increases with
age.
10-12% of the population aged over 85
years will develop dementia.
AD is more common in people with
Down’s Syndrome than in the general
population, and can occur at an earlier
age.
198.
What Causes Dementia?
There are different forms of dementia
and each has its own causes. Some of
the most common forms of dementia are:
Alzheimer’s Disease
Vascular dementia
Frontal Lobe dementia
Dementia with Lewy Bodies
199.
Delirium
Is a condition with a PHYSICAL cause
Is the most common cause of a
sudden change in behaviour
Is often managed inappropriately
Should be treated as a medical
emergency
Clues can be
A sudden change in mental state or
behaviour
A recent medication change
Infection (evidence)
Visual or tactile hallucinations
200.
Causes of Delirium
Effects of medication
Infections
Strokes
Lack of oxygen
Metabolic or endocrine problems
Trauma
Alcohol / drug withdrawal
Epilepsy
Constipation
201.
Signs & Symptoms of Delirium
Acute onset (less than 48 hours)
Clouded consciousness
Disorientation to time, place & person
Misinterpretation of environment
Restlessness / Daytime Drowsiness
Easily startled
202.
Signs & Symptoms of Delirium
Lability of mood
Hallucinations & delusions
Symptoms fluctuate
Confusion worsens at night
(nightmares)
Disturbed sleep / wake cycle
203.
General Management Principles for Delirium
Investigate and treat underlying medical cause
Pharmacological Management
Behavioural Management
Reassure and provide clear explanations for
family and care givers
204.
MENTAL HEALTH AGENTS
Johncy Joseph, RN-BSN, MBA
Avenir NCLEX , LLC
205.
MENTAL HEALTH Pharm
Antipsychotics:
Typical:
Haldoperidol (Haldol) Fluphenazine (Prolixin)
Chlopromazine (Thorazine) Thioridazine (Mellaril)
Atypical:
Risperidone (Risperdal) Quetiapine (Seroquel)
Clozapine (Clozaril) Olanzapine (Zyprexa)
Monitor for seizures
Extrapyramidal symptoms: tardive dyskinesia (involuntary movements/less likely to
occur with atypicals), parkinsonism (tremors/rigidity), akathisia (body restlessness),
dystonia (treat with antihistamines- Benadryl (Antidote))
Zyprexa: monitor for orthostatic hypotension; weight gain (also Clozapine) also used
for Bipolar Disorder.
Anticholinergic effects - dry mouth, blurred vision, constipation
Photosensitivity
Agranulocytosis may occur with Clozapine
Neuroleptic Malignant Syndrome - fever, tremor, elevated blood pressure, & heart
rate - if untreated, this is potentially fatal.
206.
The nurse is assessing a client who recently began
taking a typical antipsychotic medication. The
client says, “All of a sudden I can’t breathe right.
“The nurse observes generalized body rigidity and
diaphoresis. The body temperature is 103 degrees
F, 39 degrees C, and the pulse is 130. What
should the nurse do next?
1. Administer the ordered prn anticholinergic
medication.
2 Assess the client for indications of orthostatic
hypotension.
3. Begin preparing the client for immediate
transfer to an emergency department.
4. Arrange for an additional physician’s visit later
in the day.
207.
A client is planning to be discharged from the
hospital. It is the nurse’s responsibility to educate
this client regarding his prescribed medications.
This client is taking Clozapine (Clozaril). The nurse
makes it a priority to teach the client to notify the
physician immediately if there are:
1. Feelings of increased energy and interest in the
environment
2. Unusual reactions to exposures to the sun
3. Interferences with the normal sleep pattern
4. Indications of any sort of infection.
208.
Considering the anticholinergic side effects of
many psychotropic drugs, the nurse should
encourage clients taking these drugs to:
1. Suck on hard candy
2. Restrict their fluid intake
3. Eat a high diet in carbohydrates
4. Avoid products that contain aspirin
209.
A client has been on a typical antipsychotic
fluphenazine (Prolixin) for 12 months. When the
client comes into the Community Mental Health
Center, the nurse observes that the client has
fine, worm-like tongue movements. Which of the
following might this behavior indicate?
1. Early symptoms of tardive dyskinesia (TD)
2. A drug-food reaction, probably to grapefruit juice
3. The client has missed several doses of
medication
4. Early symptoms of neuroleptic malignant
syndrome (NMS)
210.
A client who is taking chlorpromazine
(Thorazine) is preparing for discharge. When
developing a health promotion plan for the
client, the nurse instructs the client to:
1. Avoid prolonged exposure to the sun.
2. Adhere to a strict tyramine –restricted diet.
3. Recognize the signs and symptoms of relapse
of depression.
4. Have therapeutic blood levels drawn, because
the medication has a narrow therapeutic
range.
211.
MENTAL HEALTH AGENTS
Mood disorders: Bipolar Disorder
lithium (Lithobid)
lamotrigine (Lamictal)
divalproex (Depakote)
Monitor lithium levels; Therapeutic levels: 0.5 – 1.5
mEq/L; assess for toxicity: vomiting, diarrhea,
drowsiness, decreased coordination, muscle weakness
Monitor intake/output: if sodium levels decrease,
toxicity risk increases
Monitor for seizures and arrhythmias.
Monitor for rash/Stevens-Johnson syndrome
Lamotrigine (Lamictal)
212.
The physician plans to have a client continue on
lithium after discharge. The nurse would recognize
that the teaching about the medication plan was
understood when the client states, “I know that this
medication:
1. Should be stopped if illness is suspected.”
2. May need to be taken for the rest of my life.”
3. Must be increased at the first sign of manic
episode.”
4. Rarely causes serious side effects when taken
correctly.”
213.
The nurse is evaluating lab test results for a client prescribed
lithium carbonate (lithium). The client’s lithium level is
1.9MEq/L. Which nursing intervention takes priority?
a) Give the next dose because lithium level is
normal for acute mania.
b) Hold the next dose, and continue the
medication as prescribed the following day.
c) Give the next dose after assessing for signs
and symptoms of lithium toxicity.
d) Immediately notify the physician, and hold
the dose until instructed further.
214.
A client is taking lithium carbonate (Lithium) for the
treatment of bipolar disorder. Which assessment
question would the nurse ask the client to
determine early lithium toxicity?
1. “Do you have frequent headaches?”
2. “Have you noted excessive urination?”
3. “Have you been experiencing leg aches over the
past few days?”
4. “Have you been experiencing any nausea,
vomiting, or diarrhea?”
215.
A nurse is caring for a client taking a maintenance
dosage of (Eskalith) lithium carbonate. The nurse
plans to:
1. Perform a weekly EKG.
2. Monitor intake and output.
3. Monitor daily lithium levels.
4. Observe for remission of depressive states.
216.
A nurse has provided home care instructions to a
client who is taking lithium carbonate (Eskalith).
Which client statement indicates that the client
understands the prescribed regimen?
1. “I will restrict my salt intake.”
2. “I will make sure my diet contains salt.”
3. “I keep my medication in the refrigerator.”
4. “I will be careful to avoid foods high in
potassium.”
217.
A client on an in-patient psychiatric unit is being discharged on lamotrigine
(Lamictal) 50 mg QD. After client teaching, which client statement reflects
understanding of important information related lamotrigine?
a) “I will notify my doctor immediately if I develop a
rash.”
b) “I will schedule an appointment for my blood to
be drawn at the lab next week.”
c) “I will call the doctor immediately if my
temperature rises above 102 degrees F.”
d) “I will stop my medication if I start having muscle
rigidity of my face or neck.”
218.
MENTAL HEALTH PHARM.
Mood disorders: Depression:
Selective Serotonin Reuptake Inhibitors (SSRIs)
citalopram (Celexa)
escitalopram (Lexapro)
paroxetine (Paxil)
fluoxetine (Prozac) – also used for OCD
sertaline (Zoloft) – also used for OCD
Monitor for insomnia, tremors , restlessness, sweating , constipation,
nausea, dry mouth, weight gain, headache, and sexual dysfunction.
Seratonin Syndrome - may occur with MAOIs; autonomic
instability, sweating, agitation, confusion, hyperreflexia, rigidity,
hallucinations, fever, seizures, coma
219.
The adolescent client is depressed. The client’s
ordered medication is Fluoxetine (Prozac). Which of
the following is the best response by the nurse
when the client says,” What will this medicine do
inside my brain?”
1. “It will help you feel less depressed.”
2. “It will regulate a neurotransmitter called
serotonin.”
3. “It will raise your level of the brain hormone
norepinephrine,”
4. “It will balance blood glucose and dopamine
levels.”
220.
Fluoxetine hydrochloride (Prozac) is prescribed for a
client with depression. The nurse provides instructions
to the client regarding the administration of the
medication. Which statement by the client indicates
an understanding of the medication administration?
1. “I should take the medication with my evening
meal.”
2. “I should take my medication at noon with my
antacid.”
3. “I should take the medication first thing in the
morning when I awake.”
4. “I should take the medication right before bedtime
with a snack.”
221.
Sertraline (Zoloft) is prescribed for a client in the
treatment of depression. Before administering the
medication, the nurse reviews the client’s record
and consults with the physician if which of the
following were noted?
1. A history of diabetes mellitus
2. Use of phenelzine sulfate (Nardil)
3. A history of myocardial infarction
4. A history of irritable bowel syndrome
222.
The client with a major depressive disorder
taking the selective serotonin reuptake
inhibitor (SSRI) fluoxetine (Prozac) calls the
psychiatric clinic and reports feeling confused
and restless and having an elevated
temperature. Which action should the
psychiatric nurse take?
1. Determine if the client has flulike symptoms
2. Instruct the client to stop taking the SSRI
3. Recommend the client take the medication
at night.
4. Explain that these are expected side effects
223.
The client diagnosed with a major depressive
disorder asks the nurse, "Why did my
psychiatrist prescribe an SSRI medication
rather than one of the other types of anti-
depressants?" Which statement by the nurse
would be most appropriate?
1. "Probably it is the medication that your
insurance will pay for"
2. "You should ask your psychiatrist why the
SSRI was ordered"
3. "SSRIs have fewer side effects than the
other classifications"
4. "The SSRI medications work faster than the
other medications"
224.
Serotonin/Norepinephrine Reuptake
Venalafaxine
Duloxetine
Desvenlafaxine
Levomilnacipran
Note: Everything same as SSRI
Note: Nefazodone- Serotonin Modulators- Works
same as SSRI
225.
Theclient diagnosed with pneumonia is
admitted to the medical unit. The nurse
notes the client is taking an antidepressant
medication. Which data best indicate the
antidepressant therapy is effective?
1. The client reports a "2" on a 1-10 scale,
with 10 being very depressed
2. The client reports not feeling very
depressed today
3. The client gets out of bed and completes
activities of daily living
4. The client eats 90% of all meals that are
served during the shift
226.
The client with major depressive disorder is
prescribed nefazodone (Serzone), an atypical
antidepressant. The client tells the nurse, "I am
going to take my medication at night instead of in
the morning." Which statement would be the
nurse's best response?
1. "You really should take the medication in the
morning for the best results"
2. "It is all right to take the medication at night. It
may help you sleep at night"
3. "The medication should be taken with food so
you should not take it at night"
4. "Have you discussed taking the medication at
night with your pyschiatrist” ?
227.
Tricyclic Antidepressants: Block the reuptake of Norepinephrine and serotonin
Example: SE:
Amitriptyline • Same as anticholinergic effects
Amoxapine • Sexual Dysfunction
Clomipramine • Reduce seizure threshold
Doxepin • Reduces the effect of
Imipramine Antihypertensives
Nortriptyline • Overdose – Life threatening
Trimipramine Arrhythmias- Vfib, Vtach
Change in MS
Seizures
Respiratory Failure
228.
The client with major depressive disorder
is suicidal. The client was prescribed the
tricyclic antidepressant imipramine
(Tofranil) 3 weeks ago. Which priority
intervention should the nurse implement?
1. Determine if the client has a plan to
commit suicide
2. Assess if the client is sleeping better at
night
3. Ask the family if the client still wants to
kill himself or herself
4. Observe the client for signs of wanting
to commit suicide
229.
The client with major depressive disorder has
been taking amitriptyline (Elavil), a tricyclic
antidepressant, for more than 1 year. The
client tells the psychiatric clinic nurse that
the client wants to quit taking the
antidepressant. Which intervention is most
important for the nurse to discuss with the
client?
1. Ask questions to determine if the client is
still depressed
2. Ask the client why he or she wants to stop
taking the medication
3. Tell the client to notify the HCP before
stopping medication
230.
MENTAL HEALTH PHARM.
Mood disorders: Depression:
MAO Inhibitors (Monoamine Oxidase Inhibitors)
Phenelzine (Nardil)
Tranylcypromine (Parnate)
Isocarboxide (Marplan)
Monitor for seizures and hypertensive crisis.
MAO inhibitors interact with many foods and drugs. Client is
placed on a tyramine restricted diet: NO aged cheeses,
processed or organ meats, wine, chocolate, yogurt, beer.
They are generally used as second line for depression if the
SSRIs fail.
231.
Tyramine-Rich Foods
Avocados Processed meats
Banana Overripe fruits
Beef or chicken liver-
Papaya
organ meat
Pickled herring
Raisings
Brewer’s yeast
Red wine, beer, sherry
Broad beans Sauerkraut
Aged cheese except Sausage, bologna,
cottage cheese pepperoni, salami
Eggplant Sour cream
Figs Soy sauce
Fava Beans Yogurt
232.
When Phenalzine (Nardil) or Isocarboxide (Marplan)
is administered, what must the nurse know about
the effects of these drugs?
1. Threshold for seizures is lowered.
2. Effects are potentiated when taken with other
drugs and many common foods.
3. Musculature contractions are decreased.
4. Obstructive jaundice commonly occurs.
233.
Theclient diagnosed with depression is
prescribed phenelzine (Nardil), a
monoamine oxidase (MAO) inhibitor. Which
statement by the client indicates to the
nurse the medication teaching is effective?
1. "I am taking the herb ginseng to help
my attention span"
2. "I drink extra fluids, especially coffee
and iced tea"
3. "I am eating three well-balanced meals
a day"
4. "At a family cookout I had chicken
instead of a hotdog"
234.
A client who is receiving an MAO inhibitor is going
home on a weekend pass. Considering this drug,
the nurse plans to caution the client to avoid:
1. Pork, spinach, and fresh oysters
2. Milk, peanut butter, and meat tenderizers
3. Cheese, beer, and products with chocolate
4. Orange drinks, fresh apples, and ice cream
235.
Which situation would place a client at high
risk for life-threatening hypertensive crisis?
1. A client is prescribed tranylcypromine (Parnate)
and eats chicken salad.
2. A client is prescribed isocarboxazid (Marplan)
and drinks hot chocolate.
3. A client is prescribed venlafaxine (Effexor) and
drinks wine.
4. A client is prescribed phenelzine (Nardil) and
eats fresh roasted chicken.
236.
A client on an in-patient psychiatric unit has been prescribed
tranylcypromine (Parnate) 30mg QD. Which client statement
indicates that discharge teaching has been successful?
a) “I can’t wait to order liver and fava beans
with a nice Chianti.”
b) “Chicken teriyaki with soy sauce, and tea
sound great.”
c) “I have been craving a hamburger with
lettuce and onion, potato chips, and milk.”
d) “For lunch tomorrow I’m having bologna and
cheese, a banana, and a cola.”
237.
MENTAL HEALTH PHARM.
Antianxiety meds: Benzodiazepines
Lorazepam (Ativan)
Alprazolam (Xanax)
Triazolam (Halcion)
Monitor for impaired memory, coordination or
attention; sexual dysfunction; drowsiness, dizziness
psychological and physical dependence
avoid abrupt withdrawal as this can lead to
seizures.
238.
An antianxiety medication is prescribed for an
extremely anxious client. The client states, “I’m
afraid to take these pills because I heard they’re
addicting.” The nurse’s response is based on the
knowledge that antianxiety medications:
1. Rarely causes dependence when dosage is
controlled.
2. May result in psychologic but not physiologic
dependence.
3. May require increased dosage but rarely cause
dependence.
4. Have the potential for physiologic and psychologic
dependence.
239.
The client is taking triazolam (Halcion) to reduce
anxiety related symptoms. Which client statement
indicates the nurse should provide more teaching?
1. “The physician wants me to take this drug at
bedtime because it will help me to sleep better.”
2. “I should not abruptly stop taking this
medication.”
3. “I might not be able to drive while I am taking this
medication.”
4. “I will probably have to take this medication for
the rest of my life.”
240.
In addition to hydration during delirium tremens, the
physician prescribes parenteral administration of
lorazepam (Ativan) for the client. The nurse
understands that this drug is given during
detoxification primarily to:
1. Prevent physical injury to the client when seizures
occur.
2. Enable the client to sleep and eat better during
periods of agitation.
3. Quiet the client and encourage cooperation and
acceptance of treatment.
4. Reduce the anxiety-tremor state and prevent more
serious withdrawal symptoms.
241.
MENTAL HEALTH PHARM
Alzheimer's Dementia
donepezil (Aricept)
memantine (Namenda)
galantamine (Razadyne)
Monitor for dizziness and headache; GI upset; fewest
side effects with Namenda.
242.
The client with dementia is receiving the following
medications. An unlicensed assistant who is
enrolled in nursing school asks the nurse, “Which
medication may lead to recovery of some mental
functioning by increasing acetylcholine in the nerve
synapse? The nurse responds, “The medication that
does that is:
1. Fluoxetine (Prozac)
2. Trazadone (Desyrel)
3. Haloperidol (Haldol)
4. Donepezil (Aricept)
243.
MENTAL HEALTH PHARM
Alcoholism
Disulfuram (Antabuse) is prescribed for a client who is
seen in the psychiatric health care clinic. The nurse is
collecting data from the client and providing
instructions regarding the use of this medication. Which
data is important for the nurse to obtain before
beginning the administration of this medication?
1. When the last full meal was consumed.
2. When the last alcoholic drink was consumed.
3. If the client has a history of diabetes insipidus
4. If the client has a history of hyperthyroidism.
244.
MENTAL HEALTH PHARM.
Attention Deficit Hyperactive Disorder
methylphenidate (Concerta, Ritalin)
Given to children with ADHD. Monitor for
hyperactivity, insomnia, tremor, hypertension,
tachycardia, anorexia.
245.
The client is a child with Attention Deficit
Hyperactivity Disorder (ADHD) who is receiving
methylphenidate (Ritalin ). The nurse teaches the
parents to carefully monitor which of the following
in the child?
1. Dental health
2. Oral mucous membranes
3. Height and weight
4. Milk consumption
246.
Methyphenidate (Ritalin) is prescribed to a
child with attention deficit hyperactivity
disorder (ADHD). The nurse providing
information to the mother regarding the
administration of the medication instructs the
mother to administer the medication:
1. Before dinner and at bedtime
2. At the noontime and evening meals
3. In the morning after breakfast and at
bedtime.
4. Before breakfast and before the noontime
meal.