Contributed by:
Maternity nursing reviewing was developed to understand the principles of nursing care for clients who are experiencing childbirth. The course is developed in three sections- Antepartum, Intrapartum,& Postpartum.
1.
Maternity Nursing
Johncy Joseph, RN-BSN, CMSRN, MBA
Avenir Solutions, LLC
2.
• Amniotic Fluid: Pale, Straw-Colored, fluid in which the fluid floats- Cushion
• Ballottement: Rebounding of the fetus against the examiner’s finger palpation.
• Chadwick’s Sign: Violet coloration of the mucous membrane of the cervix, vagina,
& vulva @ 4wks due to increased vascularization due to pregnancy (probable
sign).
• Goodell’s Sign: Softening of the cervix that occurs at the beginning of the second
month of pregnancy. Probable sign of Pregnancy.
• Hegar’s Sign: Compressibility and softening of the lower uterine segment that
occurs at week 6 of gestation.
• Lecithin-to-Sphingomyelin (L/S) Ratio: Lung maturity of the fetus- 2 components
of amniotic fluid. 2:1
• Lochia: Uterus discharge from placental site vessels and debris from decidua. 2-6
weeks
3.
• Nagele’s Rule: Subrtract 3 months and add 7 days to the first day of the last menses and then
add 1 year. Or Add 7 days to the last menses and count forward 9 months from that day.
• Quickening: Maternal perception of fetal movement for the first time occurring usually in the
16-20th week.
• Surfactant: Phospholipid that is necessary to keep the fetal lung alveoli from collapsing-
amount sufficient after 32 weeks.
• Placenta: Organ that provides the exchange of nutrients and waste products between the
fetus and the mother. Produce hormones to maintain pregnancy. Aka afterbirth
• Gestation: Fertilization in the ovum- Delivery= approx. 280 days
• GTPAL
Gravidity= Number of pregnancies
T= Term Births> 37 week Delivery
P= Preterm births< 37 weeks
A= Abortions or miscarriages
L= Current Living Children
Nullpara= women with no birth more than 20 weeks/ Primipara= 1 birth/Multipara= >1
4.
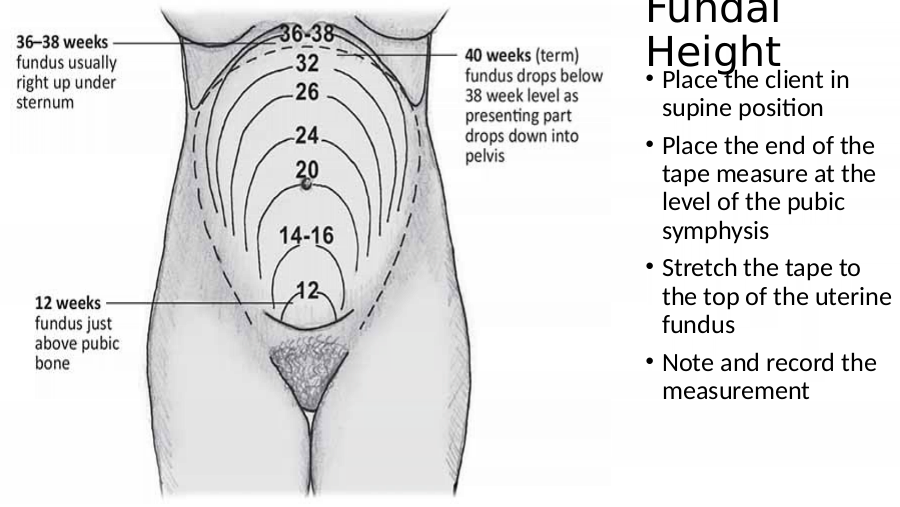
• Place the client in
supine position
• Place the end of the
tape measure at the
level of the pubic
symphysis
• Stretch the tape to
the top of the uterine
fundus
• Note and record the
measurement
5.
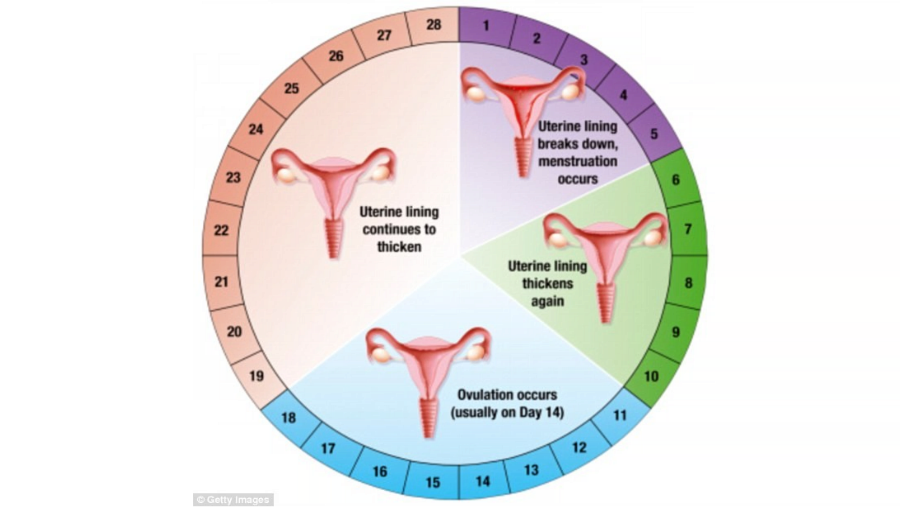
Menstrual Cycle: Four Phases
A. Menstrual Phase: Day 1- 5: Shedding of Endometrium in the form of bleeding
B. Proliferation Phase: Day 5- 14 (Ovulation begins)
C. Ovulatory Phase: FSH decrease, Progesterone increase- mature follicle aka
ovum releases from the ovary
D. Luteal Phase: Ovum travels through Fallopian tube to Uterus/Womb.
Endometrial Cycle: If the egg is not fertilized- blood supply to the egg is ceases
causing necrosis and menstruation begins- resetting to day 1
Note: Ovulation approximately 14 days before the next cycle. To avoid pregnancy a
woman should avoid unprotected sex before and the day of ovulation (most fertile
day). Typically most fertilization period begins 4-5 days before ovulation and 1-2
days after. Sperm cell can live upto 4-5 days and an egg can live 1-2 days.
7.
Indications of Ovulation
• Drop in basal body temperature 1 day before
ovulation and rise by 1 degree during ovulation
• At ovulation cervical mucus is abundant, watery
thin, clear (like egg white) known as spinnbarkeit
• Cervical Os dilates slightly, softens and rises in the
vagina
• Occasionally abdominal pain known as
mittelschmerz
• Ferning observed
8.
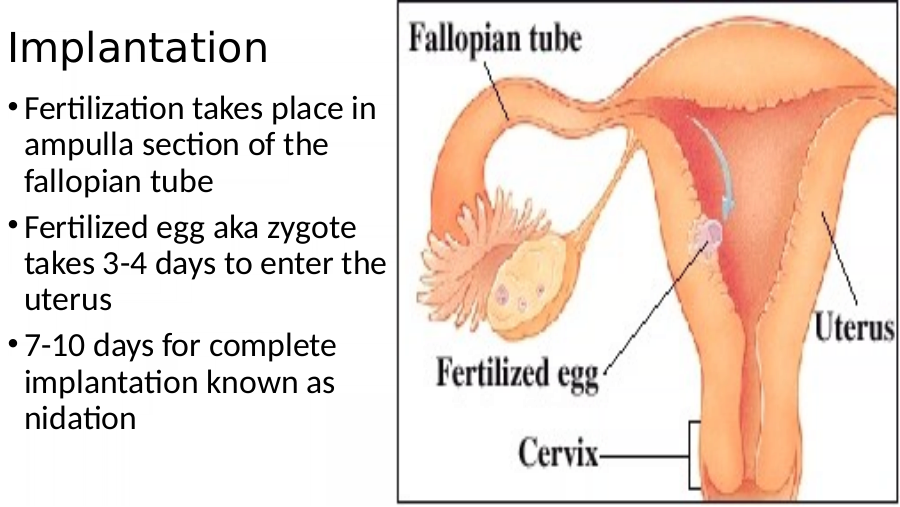
• Fertilization takes place in
ampulla section of the
fallopian tube
• Fertilized egg aka zygote
takes 3-4 days to enter the
uterus
• 7-10 days for complete
implantation known as
nidation
9.
Pregnancy Signs
• Amenorrhea- N/V
• Increased size and increased feeling of fullness in breast/pronounced nipples
• Urinary frequency
• Quickening: https://www.youtube.com/watch?v=JtWfowdzlAQ
• Hegar’s Sign
• Goodell Sign
• Chadwick Sign
• Ballottement:
• Braxton Hicks Contractions aka False Contractions- Painless contraction occurs
intermittently throughout pregnancy
• Human Chorionic Gonadotropin- HCG
10.
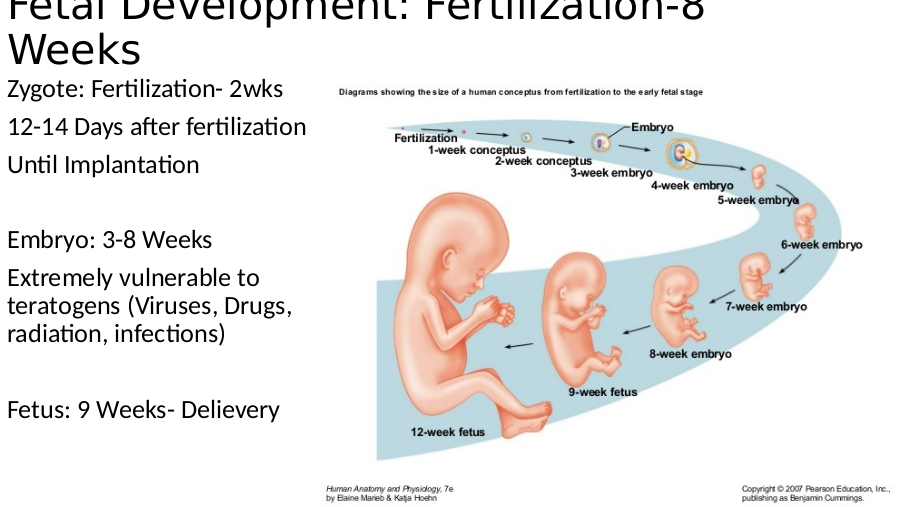
Fetal Development: Fertilization-8
Zygote: Fertilization- 2wks
12-14 Days after fertilization
Until Implantation
Embryo: 3-8 Weeks
Extremely vulnerable to
teratogens (Viruses, Drugs,
radiation, infections)
Fetus: 9 Weeks- Delievery
12.
Fetal & Maternal Changes: Week 8
Fetal Maternal
• Brain and CNS formation • Nausea- 1st trimester
• Heart begins to pump • Uterus changes from pear to globular shape
• Facial features • Hegar Sig
• Limb buds • Goodell Sign
• Ears develop from skin folds • Chadwick Sign
• Weight 2 grams • Leukorrhea Increases: a whitish or yellowish
discharge of mucus from the vagina
• Ambivalence
• Relatively no weight gain
13.
Risk Factors Associated with Pregnancy
• Age: <20-35 yrs< : High Risk
• Poor nutritional status: Should take folic acid to prevent neural tube and orofacial
clefts
• Genetic Risk Factors
• Healthcare: Failure to seek and obtain prenatal care, dental care, abuse, violence
• German Measles (Rubella): First 8 weeks
• Syphilis- (cross placenta): MR and Physical Abnormality
• Condolyma Acuminatus (HPV): Vaginal birth- Epithelial tumors in Larynx
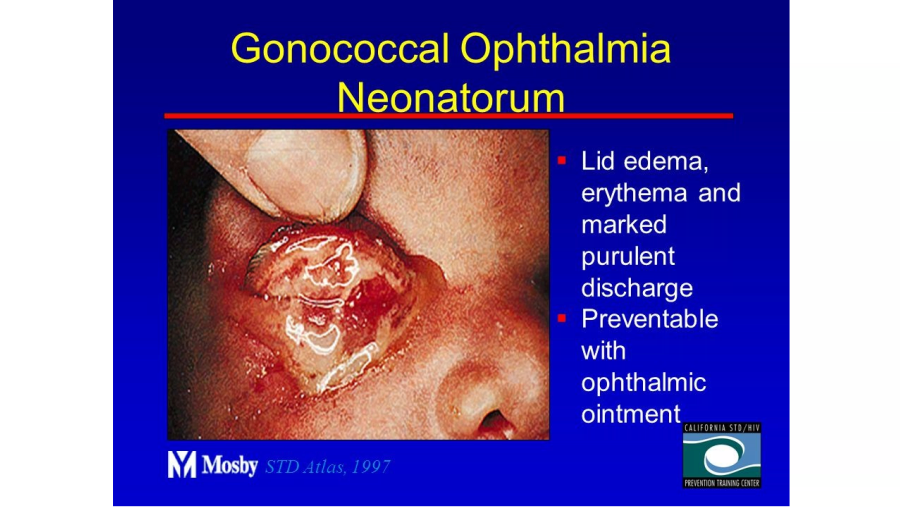
• Gonorrhea: Delivery: Opthalmia Neonatrum, PNA, & Sepsis
• Chlamydial Infection & Trichomonas: Delivery: PROM, Premature Labor, and post
partum Endometriosis
14.
Nursing Interventions for Maternal
Eat dry crackers before getting out of bed in the morning
Small, frequent meals, avoid fatty foods and avoid skipping meals
Avoid hot tubs, sauna, & steam rooms throughout pregnancy (NTD risk increase
and syncope-hypotension)
Note: DOULA is a trained labor support person employed by the patient to provide
emotional and physical labor support
15.
Fetal and Maternal Changes: 12
Weeks
Fetal Maternal
• Heart is visual with US Uterus above pelvic brim
• Lower body develops Braxton hicks are possible-
• Sex can be identified Continues throughout pregnancy
• Kidneys produce urine Weight gain 2-4 lbs
• Weight 2-4lbs Placenta functioning & producing
hormones
Risk of UTI
16.
Nursing Interventions- 12 Weeks
• Prevention of UTI
• Increase fluid intake- upto 3L/day
• Void after intercourse
• Wipe from front to the back
• Increase caloric intake by 300 C/day
• Regular exercise
• Effects of pregnancy on sexual relationship
• Identify father’s role as he recognizes parental role
17.
Fetal and Maternal Changes- 16
Fetal Maternal
• Face looks human • Quickening
• Scalp hair appears • Colostrum
• Meconium in bowel and anus • Cholesterol increases from 16-32
open weeks
• Bones and joint cavities visible • Insulin resistance starts from
with ultrasound week 14-16 and stablizies during
• Testes in position for descent the last few weeks
into scrotum or vagina open • Weight gain 1lb/week to
delievery
18.
Alpha-Fetoprotein Test: Week 16-18
• Week 16-18
• Elevated levels = Open NTD or Multiple gestations
• Low levels = Down Syndrome
19.
Fetal and Maternal Changes- 20
Weeks
Fetal Maternal
• Vernix: waxy or cheese-like • Fundus at Umbilicus
white substance found coating
the skin of newborn human • Colostrum secretion, areolae
babies darken
• Lanugo- Fine hair to protect the • Amniotic fluid 400 ml
body • Quickening
• Eye lashes, eyebrows, head hair • Nasal stuffiness, Leg cramps
• Sleeps, sucks, and kicks • Varicose veins
• Weight 11-14 oz • Constipation
20.
Nursing Interventions @ 20 Wks
• Remain active
• Feet elevated when possible
• Avoid pressure on lower thighs
• Support stockings may be helpful
• Dorsiflex to relieve leg cramps/apply heat
• Cool vaporizer or saline spray for nasal stuffiness
• High fiber diet/3 L per day fluid
21.
Fetal and Maternal Changes- 24
Fetal Maternal
• Red skin and Wrinkled-Sweat • Uterus above umbilicus
glands forming • Diastolic pressure increases from
• Blood formation in bone marrow 24-32 weeks, normalizes at term
and decreases in liver • Systolic pressure remains normal
• Alveolar sacs fromed- lecithin throughout pregnancy
appears in amniotic fluid (26-27
wks)
• Hearing begins
22.
Nursing Interventions @ 24-28 wks
• Glucose challenge test: 24-28 weeks
• US taken every 2 weeks to compare fetal growth
23.
Fetal and Maternal Changes- 28
Fetal Maternal
• Breathe, swallow, regulate • Fundus halfway between
temperature umbilicus and xiphoid process
• Surfactant forms in lungs • Abdominal breathing
• Hearing • Fetal outline is palpable
• Introspective and
• Eyelids open concentrates on the well-
• Period of greatest fetal being of unborn child
weight gain • Heartburn
• 1100 grams or 2.5 lbs • Hemorrhoids
24.
Nursing Interventions @ 28 wks
• Hemorrhoids: Sitz bath/anesthetic agents/stool
softners
• Legs elevated when sitting
• Side lying position when resting
• Eat small frequent meals/avoid fatty foods- avoid
lying down after meals
• Antacids can be given/ avoid sodium biacarbonate
• Encourage women to start childbirth classes
25.
Fetal and Maternal Changes- 32
Fetal Maternal
• Brown Fat deposition • Fundus at xiphoid process
beneath skin to insulate • Breast are full and tender
baby after birth • Urinary frequency returns
• Fetus 15-17 inches in length • Swollen ankles
• Begins storing Iron, Calcium,
• Trouble sleeping
Phosphorus
• Dyspnea
• Weighs 1800-2200 g (4-5 lb)
26.
Nursing Interventions @ 32 Wks
•Elevate leg on or two times a day
per hour
•Wear well-fitting supportive bra
•Maintain proper posture
•Sleep in a semi-fowler position at
night for dyspnea
27.
Fetal and Maternal Changes- 36-40
Fetal Maternal
• Uterus completely occupied by the Lightening
fetus Placenta- 500-550g
• Maternal antibodies transferred to Mother is eager for birth, may have
fetus for 6 months, afterwards infant’s burst of energy
own immune system
Increased backaches
• Lecithin/Sphingomyelin (L/S) Ratio- 2:1
Urinary frequency increases
• Weighs 3200 grms
Braxton hicks intensify
28.
Nursing Interventions
• Wear low heeled shoes
• Avoid heavy lifting
• Sleep on side to relieve bladder pressure and urinating
frequently
• Encourage woman to do pelvic tilt exercises
• Keep a suitcase packed
• Encourage the couple to tour L & D area
• Discuss postpartum circumstances- circumcision,
postpartum blues, birth control, rest, father’s role
29.
Physiological Changes During Pregnancy
• Pulse rate 10-15 bpm & BP decreases- 2nd
Trimester, increased respirations Psychological
• N-V due to HCG release/ Hemorrhoids due to • Ambivalence
venous pressure increase • Acceptance-
• Gingivitis & Ptyalism due to increase in Estrogen Readiness
• Increased urinary frequency • Emotional Lability-
• Chadwick’s Sign Mood swings
• Lumbosacral curve increases- waddling gait- • Body Image Concerns
RISK FOR FALL • Daydreaming to
• Syncope: Avoid Supine position (2nd & 3rd prepare for
Trimesters)- Uterus pressure on IVC motherhood
• Note: Colostrum discharge, Heart Burn, Kegel
Exercises, Ankle Edema, Varicose Veins,
Backache, leg cramps
30.
Antepartum Nursing Care: Initial Visit
• History and Physical
• Signs of healthy psychosocial bonding includes- massaging the abdomen,
nicknaming the fetus, talking to fetus in utero
• For many women, battering (emotional or physical abuse) begins during
pregnancy. Women should be assessed for abuse in private, away from the
partner by a nurse who is familiar with local resources and know how to
determine the safety of the patient.
• Calculate EDB: Nagele’s Rule
• VS: BP- 90-140/60-90, HR- 60-90, RR- 16-24, T- 36.1-37.7
• CBC with differential
• Pap smear& Cytology (gonorrhea and chalmydia)
• Antibody Screeing: HIV, HepB, Toxoplasmosis, Rubella, Syphillis, CMV , PPD, Blood
type , UA
31.
Antepartum: Subsequent Visits
• Check Urine
Albumin/Protein- Preeclampsia or Renal failure, Trace amount ok
Glucose- Gestational Diabetes
• Ist trimester- 2-4 lbs
• 2-3rd trimester- 1lb/week
• Educate patient as pregnancy advances- uterus presses on abdominal vessels, IVC
and aorta: Left lying position increases blood supply to placenta
• Dental care- Gum hypertrophy is common
• Round-ligament pain is expected
• Educate patient to come to the hospital when contractions are 5 minutes apart
32.
Antepartum: Nutrition
• Increase calorie intake by 300 C/Day
• Increase protein by 30g/day
• Drink 8-10 glasses of fluid, 4-6 glasses should be water
• Prenatal vitamins to ensure Folic acid and iron intake is adequate
• 3 servings of dairy group (milk and cheese)
• 5 servings of protein
• 5 servings of vegetables
• 6 servings of breads and cereals
• Pregnant women should consume 3 cups of milk or yogurt/day. Ensure daily
calcium intake and reduce leg cramps
33.
Diagnostic Testing
• Schedule
Q 4 Wks for upto 28-32 Wks
Q 2 Wks from 32-36 Wks
Q 1 Wk from 36-40 Wks
• Blood Type & Rh Factor:
Determine ABO typing
Rh Typing: https://www.youtube.com/watch?v=7OWp8d8WKkg
Rh+ = Presence of Antigen
Rh- = Absence of Antigen
If Client Rh Negative – Baby Rh Positive- RHOGAM at 28 Weeks Rho (D)
34.
Diagnostic Testing
• Rubella Titer
if negative (<0.8)- Should received immunization
When getting immunized- client cannot get pregnant for upto 1-3 months
If Rubella vaccine and RHOGAM administered at the same time- vaccine ineffect.
Can be administered post partum (before dc)- subq (inquired about sensitivity to
eggs)
Note: Rubella vaccine not administered during 1st trimester because live attenuated
virus can cross placenta and risk fetus development
• HgB & Hct- Decrease due to increase in plasma
• Hgb < 10 – Anemia
• Pap Smear- During initial prenatal visit to screen for Cervical Neoplasia
35.
Diagnostic Testing
• Hepatitis B Surface Antigen
• At risk individuals who should be vaccinated for Hep B
HCW
IV Drug Users/Tattos/ STDs/HD or Renal Txp
Clients born in Asia, Africa, Haiti, Pacific Islands
Individuals with undiagnosed jaundice or chronic liver disease
Note: Hep B IS NOT CONTRAINDICATED DURING PREGNANCY
• UA & UC
UA obtained every visit to determine for glucose and protein in urine
Glycosuria – Expected, WBC- Infection, Ketoneuria- malnutrition
Increased Protein (+2 to +4)- Infection or PREECLAMPSIA
36.
• Outlines and Identifies fetal and maternal structures
• Gestational Age
• Amniotic Fluid Volume (aka amniotic fluid index)
• Abdominally or transvaginally
Woman may need to drink water to fill the bladder before the ultrasound
Transavaginal – Lubricated probe
No risk to either client or fetus
37.
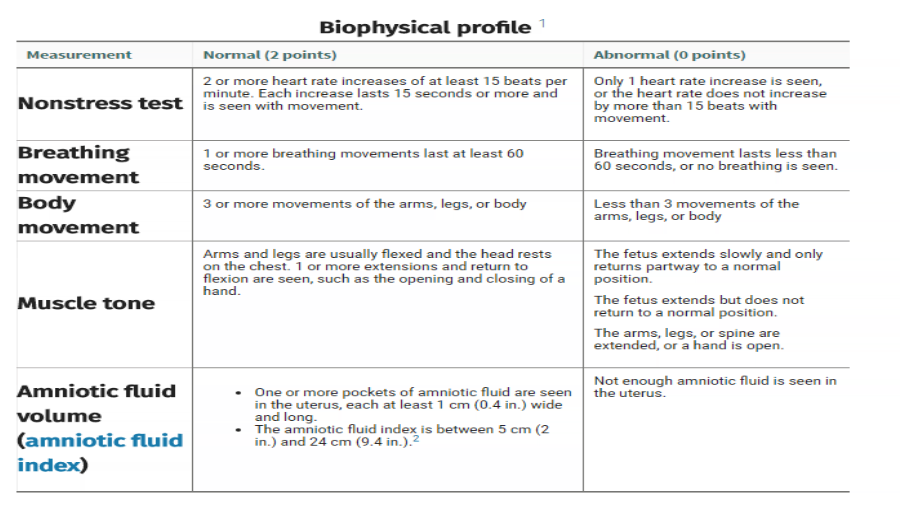
Biophysical Profile (BPP)
• Non- Invasive/Ultrasound to detect fetal well being/Non-Stress test
• Fetal movements, fetal tone, amniotic fluid index, fetal HR
• A score of 8 to 10 points means that your baby is healthy
Doppler Blood Flow Analysis: Non-invasive – Blood flow in the fetus and placenta
Percutaneous Umbilical Blood Sampling: Only when necessary- Insert the needle
directly into the fetal umbilical vessel under US guidance
Note: FHR monitoring for 1 Hr- F/Up US to ensure no bleeding or hematoma
39.
Alpha-Fetoprotein Screening
• To detect Open Neural Tube and Abdominal wall Defects
• To assess for quantity of fetal serum proteins- abnormal proteins
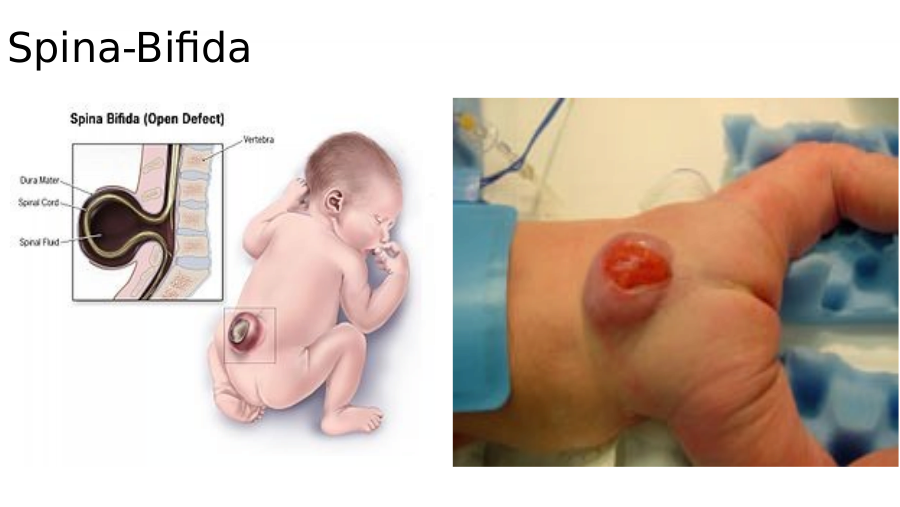
• Spina Bifida and Down Syndrome
• False Positive if common- If abnormal- repeat test
Maternal Blood test: 16-18 weeks
If level abnormal and gestation is less than 18 weeks repeat test
US to r/o fetal abnormalities
42.
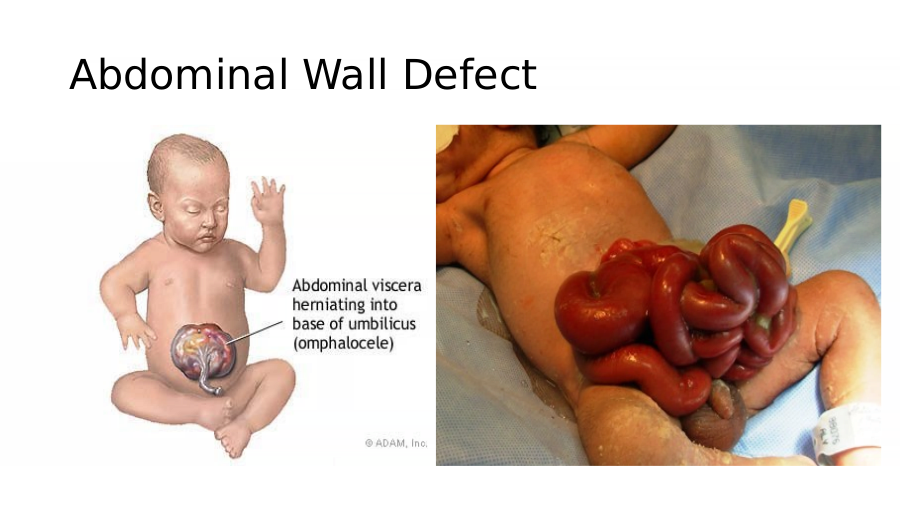
Abdominal Wall Defect
43.
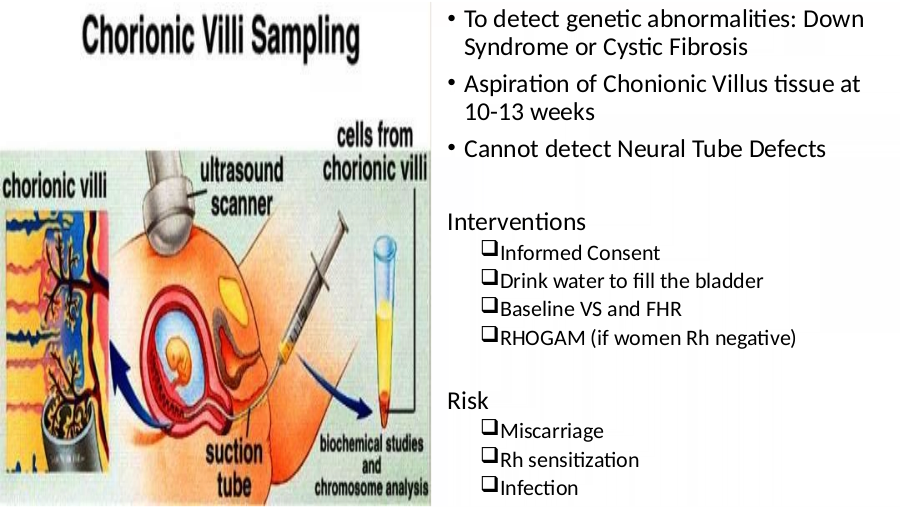
• To detect genetic abnormalities: Down
Syndrome or Cystic Fibrosis
• Aspiration of Chonionic Villus tissue at
10-13 weeks
• Cannot detect Neural Tube Defects
Informed Consent
Drink water to fill the bladder
Baseline VS and FHR
RHOGAM (if women Rh negative)
Miscarriage
Rh sensitization
Infection
44.
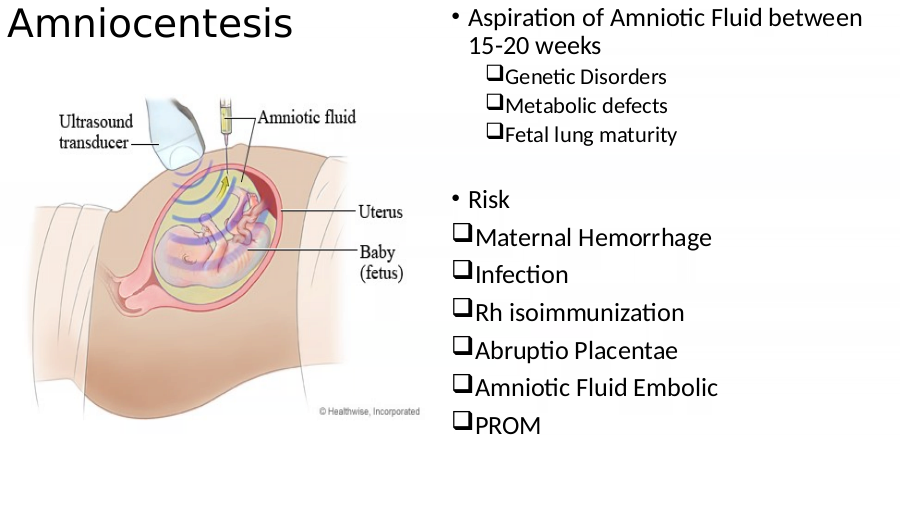
Amniocentesis • Aspiration of Amniotic Fluid between
15-20 weeks
Genetic Disorders
Metabolic defects
Fetal lung maturity
• Risk
Maternal Hemorrhage
Infection
Rh isoimmunization
Abruptio Placentae
Amniotic Fluid Embolic
PROM
45.
Amniocentesis: Interventions
• Informed Consent
• If less than 20 weeks- Client must have a full bladder
• If greater than 20 weeks- client must have an empty bladder
• Ultrasonography to locate placenta and avoid puncture
• Baseline VS and FHR- monitor q 15 minutes
Note: After CVS and Amniocentesis: Instruct client if fever, chills, bleeding, leakage
of fluid from the insertion site, decreased fetal movement, uterine contractions, or
cramping occurs – NOTIFY MD IMMEDIATELY
46.
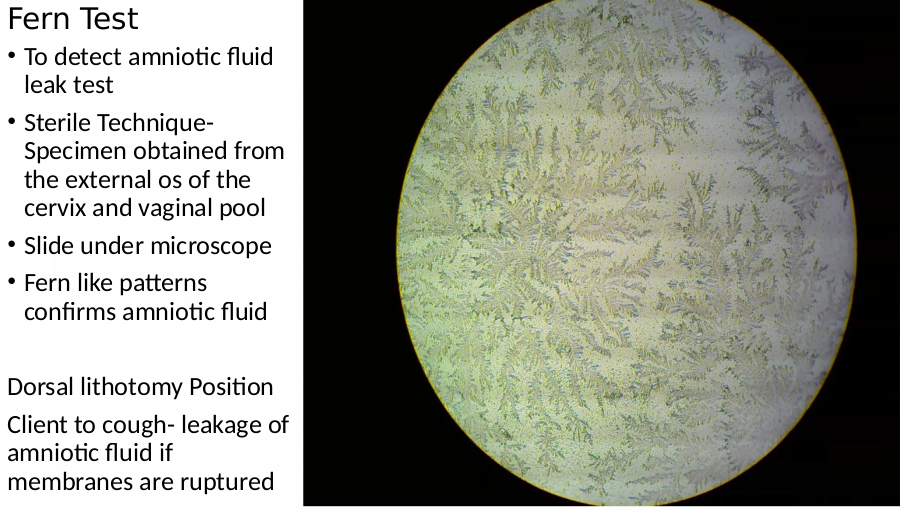
Fern Test
• To detect amniotic fluid
leak test
• Sterile Technique-
Specimen obtained from
the external os of the
cervix and vaginal pool
• Slide under microscope
• Fern like patterns
confirms amniotic fluid
Dorsal lithotomy Position
Client to cough- leakage of
amniotic fluid if
membranes are ruptured
47.
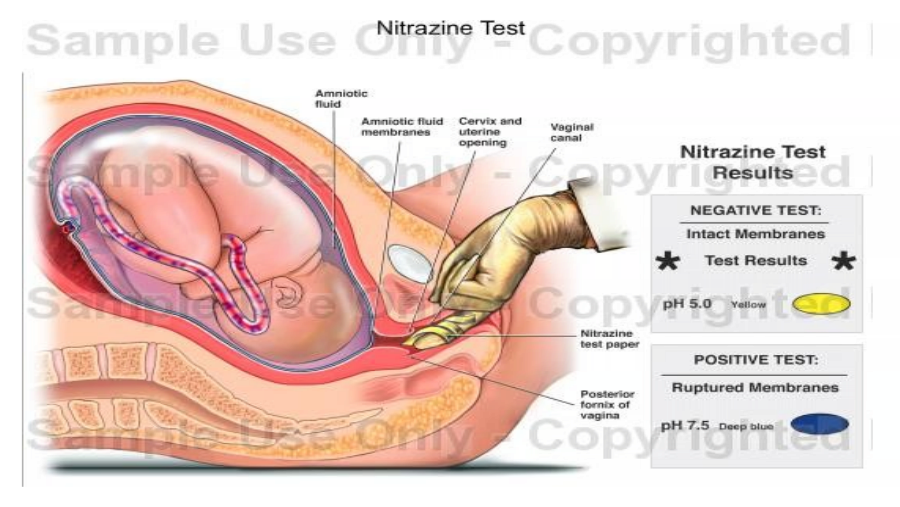
Nitrazine Test: To detect Amniotic
• Nitrazine test strip
• Vaginal Secretions pH 4.5-5.5 and will not affect the Nitrazine Strip
• Amniotic Fluid pH 7-7.5- Nitrazine test strip turns blue
Dorsal Lithothomy position
Touch the test tape to the fluid
49.
Fibronectin test: To detect premature birth
• Fetal Fibronectin a protein is found in cervical and vaginal secretions until 16-20
wks and then near term
• Postive test- Labor in 1-3 weeks
• It is only used when there is a risk of preterm< 37 weeks
Lithotomy position
Cervical secretions obtained with cotton swab
50.
Non stress Test: Fetal Well Being/US/Placental Function
• Client is placed on side lying position to avoid IVC compression
• Baseline BP and and BP throughout the procedure
• Client presses a button every time with fetal movement to record it as the point
of reference
Reactive Non-Stress Test: normal aka negative
2 or more FHR acclerations of atleast 15bpm lasting 15 seconds corresponding to
fetal movement
Nonreactive Non-Stress Test: Abnormal
Unsatisfactory: Poor quality of FHR Tracing- cannot interpreted
51.
Contraction Stress Test: To assess placental oxygenation
• Fetal well-being and if fetus can tolerate labor
• Test is performed if non-stress test is unsatisfactory
External FHR monitor- Baseline strip 20-30 minutes recorded
Oxytocin (Pitocin)- To stimulate contraction Or nipple stimulation
For three contractions with a duration of 40 seconds or more in a 10 minute period
Maternal BP monitored while increasing doses of Oxytocin
Negative Stress Test- Normal (No late decelerations of the FHR)
Positive Stress Test- Abnormal (Late Decels)
52.
• 25-35 Lbs weight gain during pregnancy
• Folic Acid high diet, 8-10 glasses of water, no restriction with Na
• Vegetarian- Deficiency in B12, Protein, Iron, Ca, Omega Fatty Acids
• Eat- Tofu, soy milk, meat substitutes, legumes, nuts, seeds, sprouts
PICA: Eating non-food substances- dirt, clay, starch, freezer frost
IRON DEFICIENCY ANEMIA
53.
Risk Condition Associated with
• Cardiac Diseases: Increased plasma • Corrected Tetratology of Fallot
volume and CO • Pulmonic or Tricuspid Disease
• Mitral Stenosis
• Assessment • Patent Ductus Arteriosus
Cough & Respiratory Congestion • Ventricular Septal Defect
Dyspnea and fatigue
Palpitations and tachycardia
Peripheral Edema
Chest Pain
54.
Risk Condition Associated with
• Chorioamnionitis: Bacterial infection of the amniotic cavity due to premature or
prolonged rupture of the membranes, vaginitis, amniocentesis
Assessment: Febrile, foul smelling amniotic fluid, leukocytosis
Gestational Diabetes Mellitus:
1st Trimester- Insulin demand increases
2nd & 3rd Trimester- Increase in placental hormones causes an insulin-resistant
state- requiring insulin decrease
Post placenta delievery- Placental hormone levels abruptly- insulin demand
Note: Newborn of diabetic mother is at risk of hypoglycemia, hyperbilirubiniemia,
respiratory distress syndrome, hypocalcaemia, congenital anomalies
55.
Gestational Diabetes
• Screening should be done between Assessment
24-28 weeks Excessive Thirst
• 3 hr oral glucose tolerance test Hunger
Weight loss
Predisposition Frequent urination
35 yrs
Blurred vision
UTI and Vaginal Yeast Infections
Multiple Pregnancies
Glycosuria and ketonuria
Family Hx
Gestational HTN
Large fetus
Polyhydramnios
Large fetus
56.
Disseminated Intravascular
Coagulation: DIC
• Rapid and extensive formation of clots that occurs in DIC causes the platelet and
clotting factors to be depleted. This causes bleeding and clotting at the same
time.
• Causes: Placental Abruption, Amniotic Embolism, Gestational HTN, Fetal death,
Liver disease, sepsis
• Assessment: Bleeding and bruising, signs of shock, occult blood
• Interventions
Remove underlying cause
VS- Bleeding and signs of shock
O2, volume replacement, heparin
57.
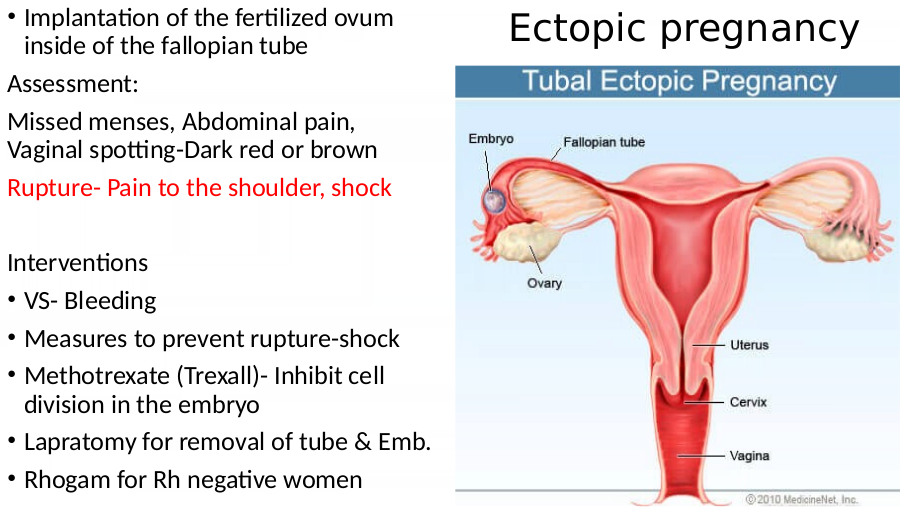
• Implantation of the fertilized ovum
inside of the fallopian tube
Ectopic pregnancy
Missed menses, Abdominal pain,
Vaginal spotting-Dark red or brown
Rupture- Pain to the shoulder, shock
• VS- Bleeding
• Measures to prevent rupture-shock
• Methotrexate (Trexall)- Inhibit cell
division in the embryo
• Lapratomy for removal of tube & Emb.
• Rhogam for Rh negative women
58.
Endometrosis: Infection of the lining
of uterus
Assessment Interventions
Chills and fevers VS
Tachycardia Fowler position to facilitate drainage of
Decreased appetite lochia
HA & Backache Private room- newborn can stay with
the mother
Tender-large uterus
Educate mother of hand washing
Foul odor to lochia- reddish brown
lochia Initiate contact precaution, if needed
Ileus AB
Elevated WBC- Left shift of immature Back rubs and positional changes
cells Psychosocial support
59.
Hypertension and Pregnancy
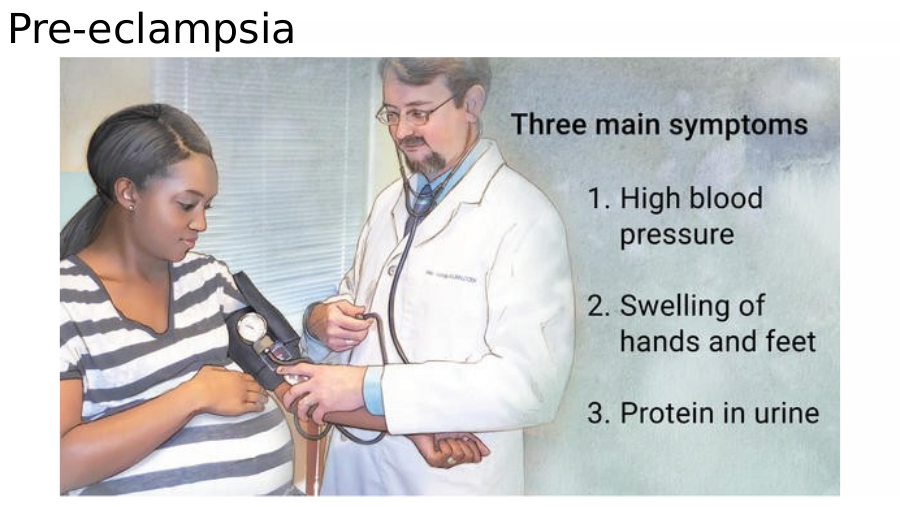
• Gestational hypertension: Interventions for Pre-eclampsia
Mild (140-160/90-110)
• Maintain bedrest
Severe (>160/110)
• Magnesium Sulfate to prevent seizures
• Pre-eclampsia: Severe HTN which can be continued for 24-48 hrs in
HTN, Proteinuria, Peripheral
postpartum
Edema
After 20 wks • Monitor for Magnesium Toxicity
• HELLP: Lab diagnosis of severe • Flushing, sweating, hTN, Depressed
preeclampsia Deep tendon reflexes, CNS Depression
Hemolysis • Antidote: Calcium Gluconate
Elevated liver enzyme levels • Antihypertensive
Low platelet count • Induction of the labor
61.
Eclampsia: Generalized
Assessment Priority Nursing Actions/Interventions
• Seizure typically begins with • Remain with the client and call for
twitching around the mouth help
• Ensure patent airway
• Body Tonic for 15-20 seconds
• Turn the client on her side
• Body Clonic for 1 minute
• O2 8-10 Lpm
• Respiration ceases during • Monitor FHR patterns
seizure because diaphragm • Anti-seizure medications
becomes rigid
• Post seizure insert an oral airway and
• Breathing resumes after seizure suction the client’s mouth as needed
• Postictal sleep occurs • Prepare for the delivery
• Document
62.
Toxoplasmosis
• Transmitted to mother through raw meat or handling of cat litter of
infected cats
• Organism crosses placenta to fetus; may cause spontaneous abortion in
first trimester
Rubella
• Teratogenic in first trimester as organism crosses placenta, causing
congenital defects of eyes, heart, brain
Cytomegalovirus
• Organism transmitted through close personal contact; crosses placenta;
fetus may also become infected during passage through birth canal
63.
Genital herpes
• Virus transmitted to fetus during birth through infected vagina or
via ascending infection after rupture of membranes; can cause
death or severe neurological impairment in newborn
• If mother has active herpes lesions
• Delivery of fetus is via cesarean section
• If lesions are only in anal, perineal, or inner thigh area, but not
vaginal area, then delivery can occur vaginally, with strict
precautions to protect fetus
64.
• Group B Streptococcus (GBS)
• Leading cause of life-threatening perinatal infections
• Transmitted to fetus during vaginal delivery; can lead to
infections of newborn such as sepsis, pneumonia,
meningitis
• Mother diagnosed via vaginal and rectal cultures between
35 and 37 weeks’ gestation; if present, antibiotics
prescribed to mother during labor and birth, with potential
IV antibiotic administration to infected infants
65.
The Process of Labor—Four P’s
Coordinated sequence of involuntary uterine contractions to
move fetus through birth canal, to delivery, actual birth of
Four major factors interact during normal childbirth; four
P’s depend on each other for safe delivery
• Powers: Uterine contractions
• Passageway: Mother’s rigid bony pelvis, soft tissues of
cervix, pelvic floor, vagina, introitus
• Passenger: Fetus, membranes, placenta
• Psyche: Woman’s emotional system
66.
Leopold’s Maneuvers
To determine presentation and position of fetus
• If head is in fundus, hard, round movable object felt; if buttocks
in fundus, then soft, irregular shape, more difficult to move
• Back of fetus should be felt on one side of abdomen
• Irregular knobs and lumps, hands, feet, elbows, and knees felt on
opposite side of abdomen
67.
True labor False labor
• Contractions increase in • Exaggeration of normal contractions
duration and intensity • Labor does not produce dilation,
• Cervical dilation, effacement, or descent
effacement are • Contractions are irregular, without
progressive progression
• Walking has no effect on
• Contractions from back contractions; often relieves false
to the front labor
68.
Breathing techniques
• Provide focus during contractions
• Promote relaxation and oxygenation
• Begin with simple breathing patterns to more
complex
69.
Mechanisms of Labor: Intrapartum Initial Assessment
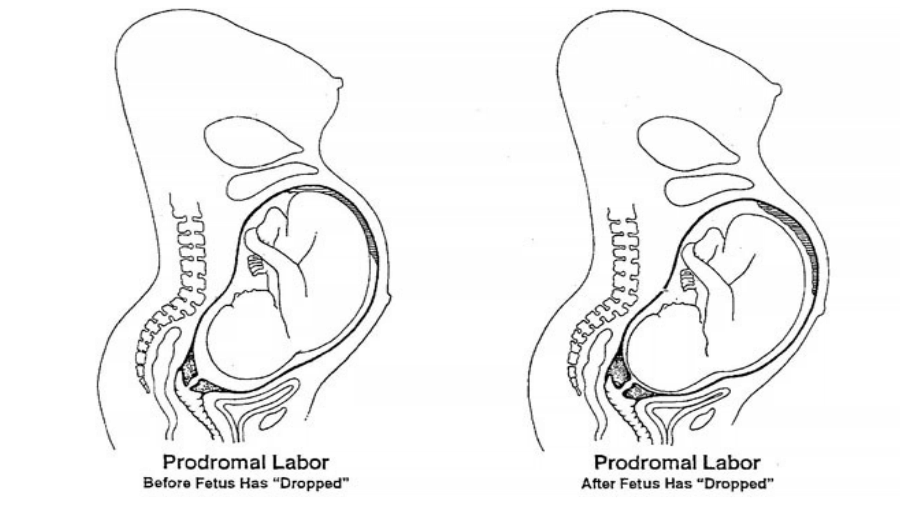
• Lightening: Fetus descends into pelvis about 2 weeks before delivery
• Braxton-Hicks contractions increase
• Vaginal show present; vaginal mucosa congested; vaginal mucus
increases
• Cervical mucus plug is passed
• Cervix ripens, becoming soft, partly effaced; may begin to dilate
• Mother has sudden burst of energy, often known as “nesting”
• Loss of 1 to 3 lb from water loss as fluid shifts secondary to
hormonal changes prior to labor
• Spontaneous rupture of membranes occurs
72.
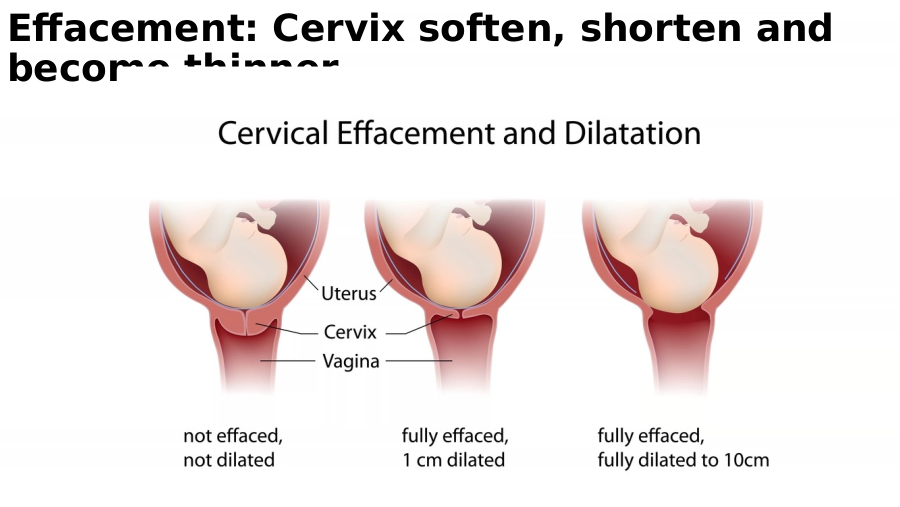
Effacement: Cervix soften, shorten and
become thinner
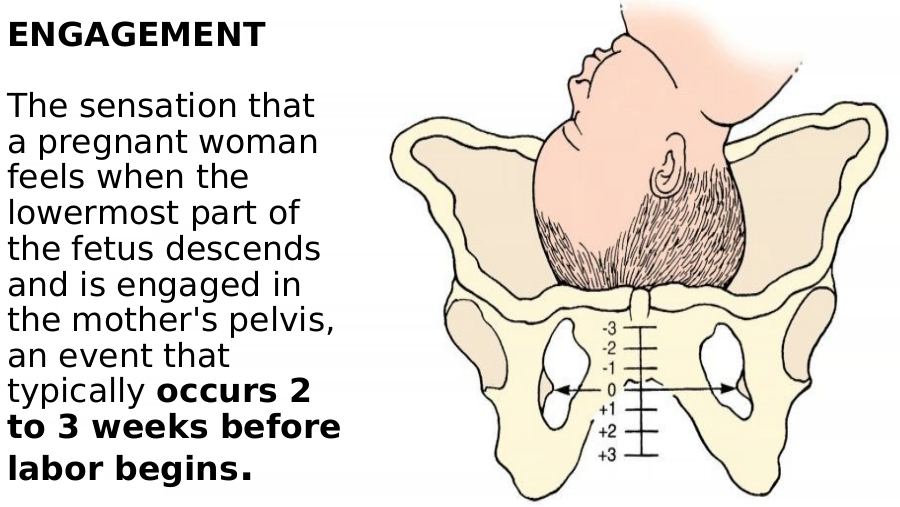
73.
The sensation that
a pregnant woman
feels when the
lowermost part of
the fetus descends
and is engaged in
the mother's pelvis,
an event that
typically occurs 2
to 3 weeks before
labor begins.
74.
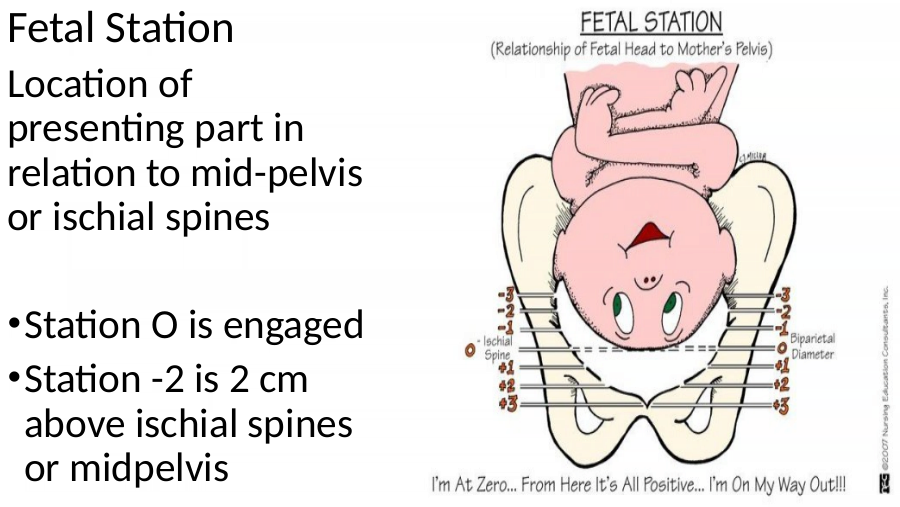
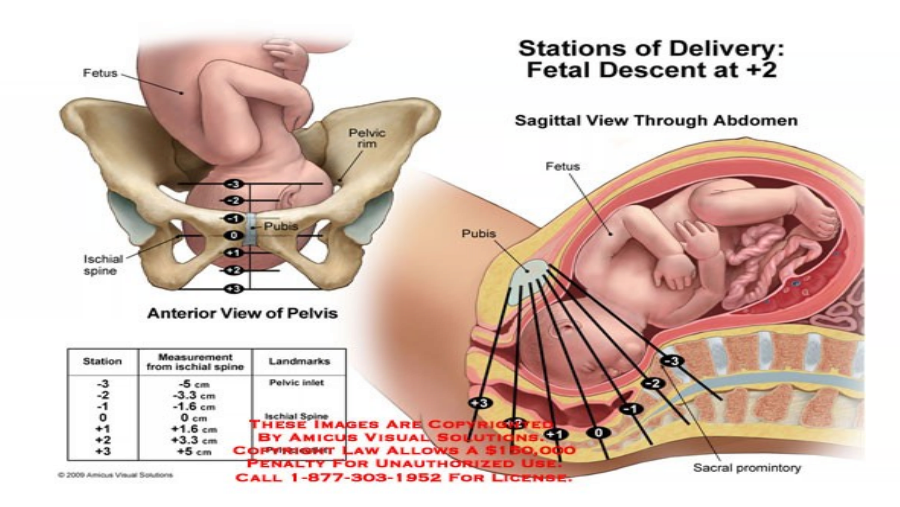
Fetal Station
Location of
presenting part in
relation to mid-pelvis
or ischial spines
• Station O is engaged
• Station -2 is 2 cm
above ischial spines
or midpelvis
76.
Four stages of labor
First Stage: Beginning of Contractions or ROM to 10
cm dilation and 100% effacement
Second Stage: 10 cm dilation to the delivery of fetus
Third Stage: Delivery of the fetus and delivery of the
placenta
Fourth Stage: 2-4 hours after the delivery of
placenta
77.
First Stage of Labor: Three Phases- 8-12 hours
Latent Phase: Beginning of true labor to 3-4 cm cervical dilation
• Mother anxious, but able to continue usual activities
• Mild contractions: 10-20 mins apart/15-20 sec duration, 5-7 min with 30-40 sec
Active Phase: From 4-7 cm cervical dilation
• Anxiety builds up with increased discomfort/Unwillingness to be left alone
• Moderate contractions: 2-3 min apart, 30-60 sec duration
Transition Phase: From 8-10 cm to complete dilation/effacement
• Behavior can be changed: extremely irritable, unwillingness to be touched, although need
company
• sudden hiccups and nausea
• Severe Contractions: 1-1.5 min apart with 60-90 sec duration
78.
Consider This during First Stage
• Watch for cord prolapse is if the infant’s head is floating
• Meconium stained fluid is yellow-green or gold-yellow- fetal stress
• Breathing techniques such as deep chest, accelerated, and cued are
not prescribed during the stage or phase of labor but by the discomfort
level of the labor.
• Monitor for Respiratory Alkalosis- Dizziness, tingling of the finger, stiff
mouth: Use paper bag for hypoventilation
• Epidural given during Active Phase (4-7cm dilation) of the labor
If too early- delay the labor
If too late- increase the risk of neonatal respiratory depression
79.
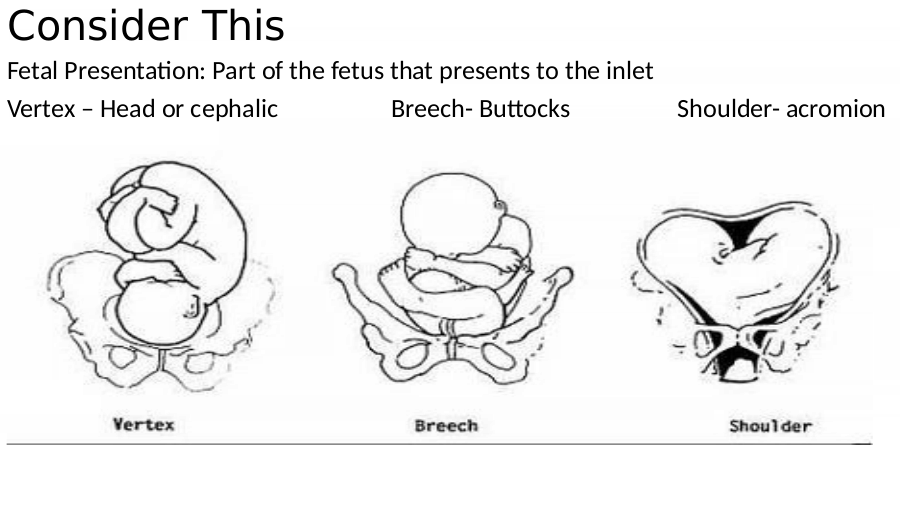
Consider This
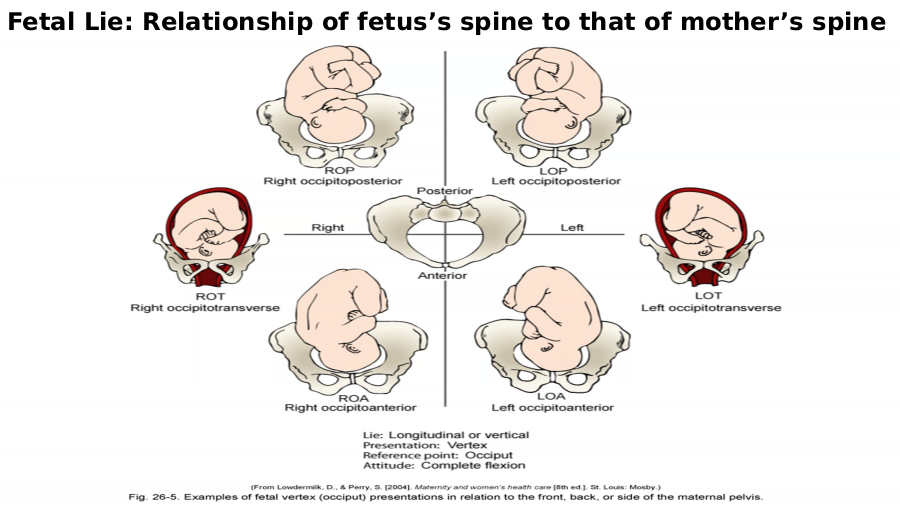
Fetal Presentation: Part of the fetus that presents to the inlet
Vertex – Head or cephalic Breech- Buttocks Shoulder- acromion
80.
Fetal Lie: Relationship of fetus’s spine to that of mother’s spine
81.
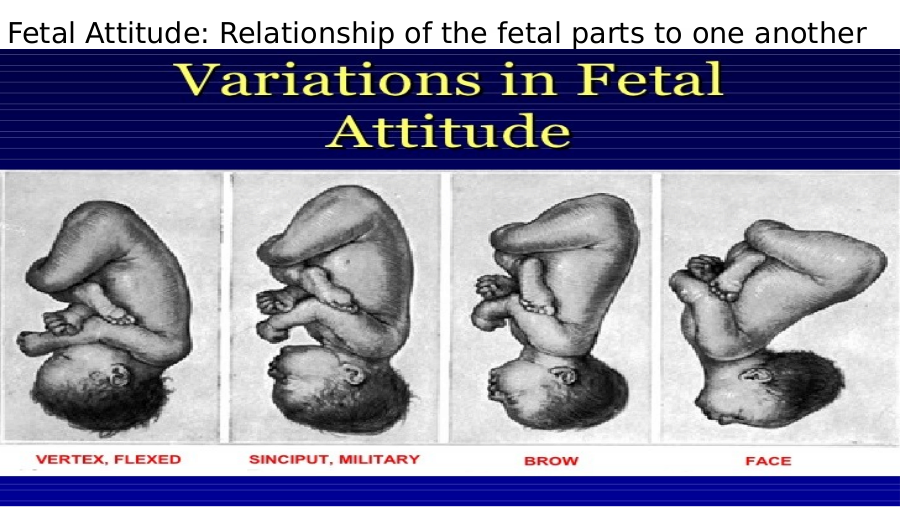
Fetal Attitude: Relationship of the fetal parts to one another
82.
Second Stage of the Labor: 1hr pgravida,
15 mins: multip
When mother involuntary needs to pushing, complete dilation of 10 cm, rapid fetal
descent and birth
• Assess BP and pulse q 5-15 minutes
• FHR with every contraction
• Perineal Area
Increase in blood show
Bulging perineum and anus
Visibility of presenting part
• Palpate for bladder distention
• Assess amniotic fluid for color and consistency
• Teach mother positions such as squatting, side-lying, high fowler, lithotomy for
pushing
83.
Second Stage of the Labor: 1hr pgravida, 15 mins: multip
• Teach mother to exhale when pushing or use ‘Gentle
Pushing Technique’
• Determine cervical dilation before allowing the client to
push- cervix should be completely dilated at 10 cm,
without it pushing can cause cervix to become swollen
and never fully dilate
• At crowning- Put gentle counter pressure against
perineum- DO NOT ALLOW RAPID DELIEVERY OVER
WOMAN’S PERINEUM
• Record delivery time- exact
84.
Crowning: Showing of head through
vaginal opening
85.
Third Stage of Labor: 5-15 Minutes
• Note: Longer the third stage- greater the risk of uterine
atony/hemorrhage
• Assess for Placental Separation
Lengthening of umbilical Cord outside vagina
Gush of blood
Uterus changes from oval (discoid) to globular
Mother describes a “full” feeling in vagina
Firm uterine contractions continue
86.
Third Stage of Labor: 5-15 Minutes
• Place hand under drape and palpate fundus of uterus for firmness and placement
at or below the umbilicus.
• Signs of placental separation- aske mother to push gently
• Take maternal BP before and after placental separation
• Administer uterine stimulants after delivery of placenta
• Monitor blood loss and track EBL
• Dry, suction infant, perform APGAR, place blanket on mother’s abdomen and
allow skin-to-skin contact with mother after delievery
• Cover head with to prevent heat loss
• Allow father to hold infant during repair of episiotomy, also siblings if possible
87.
Fourth Stage of Labor: 1-4 hrs after
• Maintain bed rest for atleast 2 hours to prevent orthostatic hypotension
• VS
Q 15 mins for 1 hr
Q 30 mins until stable
Temperature: > 38 degree- Notify MD and monitor hourly
• Assess fundal firmness and height, bladder, lochia, perineum every 15 for 1 hour
and every 30 mins for 2 hours
• Fundus- Firm, midline, at or below the umbilicus- EXPECTED
IF SOFT OR BOGGY- MASSAGE/RUB THE FUNDUS
IF ABOVE UMBILICUS OR RIGHT SIDE- SUSPECT FULL BLADDER
FIRST MASSAGE THE FUNDUS- PATIENT VOID-RECHECK FUNDUS Q 15 MINS
FOR 1 HR AND 30 MINS FOR 2 HRS
88.
Uterine Stimulants
Oxytocin: Uterine atony- Side effects: Severe afterpains in multipara, HTN
• Give immediately after delivery of placenta to avoid “trapped” placenta
• Continue to monitor vaginal bleeding
• May stimulate let-down milk reflex and flow of milk engorged
Methlyergonovine Maleate: Uterine Atony: SE- HTN
• Caution with HTN or preclampsia
• BP>140/90, hold and notify MD
Prostaglandin F2: Uterine Atony: SE- HA, N-V, Febrile, Bronchospasm/wheezing
• Contraindicated for Asthma, may be given intramyometrially by provider
• Temperature q 1-2 hrs, Auscultate breath sounds
89.
Consider This
Notify MD
• VS abnormal
• Uterus not becoming firm with massage
• Second Perineal Pad soaked in 15 minutes
• Signs of Hypovolemic Shock- Pale, Clammy, tachy, Lightheaded, hTN
Keep bladder empty- Catherize only if needed
Keep side rails up and call light within reach- instruct client not to get OOB
Apply ice pack to perineum to minimize edema- episiotomy (3 or 4th degree)
Hazel compress
Support parental emotional needs and promote bonding
Openly share in the joy and excitement of child birth, and grieve with loss
Provide a warm, darkened environment for newborns eyes
90.
Fetal Monitoring
Means of assessing fetal heart rate (FHR) as it relates to uterine contractions
Normal FHR 120 to 160 beats/min
• External fetal monitoring
• Noninvasive; performed using tocotransducer or Doppler ultrasonic transducer; transducer, fastened
with belt, should be placed on side of mother where fetal back is located (find using Leopold’s
manuevers)
• Internal fetal monitoring
• Invasive; requires rupturing of membranes; attachment of electrode to presenting part of fetus; mother
must be dilated 2 to 3 cm to perform this procedure
• Periodic patterns in FHR
• If change occurs, turn mother to left side, administer oxygen as prescribed
• Accelerations may occur with fetal movement or contractions
• Early decelerations occur during contractions when fetal head is pressed against woman’s pelvis; require
no intervention
• Late decelerations usually associated with impaired placental exchange or uteroplacental insufficiency;
require interventions to improve placental blood flow and fetal oxygenation, including immediate
delivery of fetus
• Variable decelerations usually caused by umbilical cord compression; require change in maternal
positioning
91.
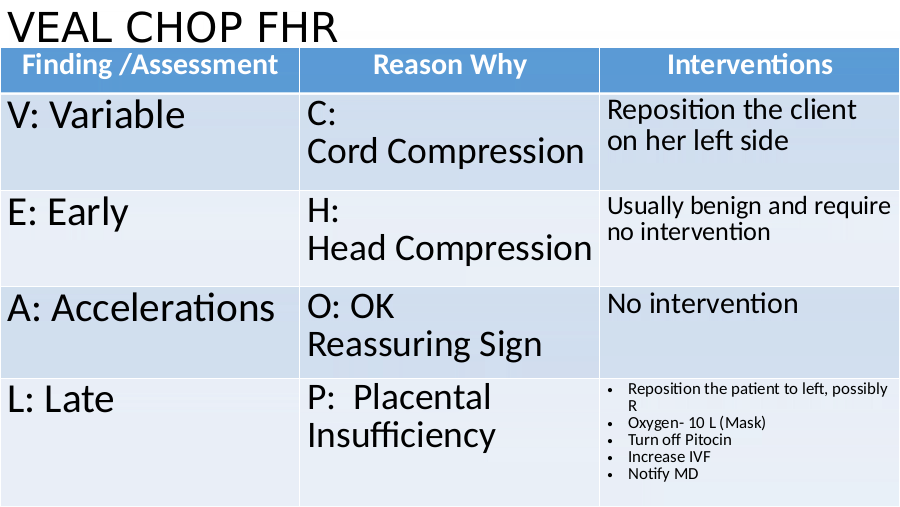
VEAL CHOP FHR
Finding /Assessment Reason Why Interventions
V: Variable C: Reposition the client
Cord Compression on her left side
E: Early H: Usually benign and require
no intervention
Head Compression
A: Accelerations O: OK No intervention
Reassuring Sign
L: Late P: Placental • Reposition the patient to left, possibly
R
Insufficiency • Oxygen- 10 L (Mask)
• Turn off Pitocin
• Increase IVF
• Notify MD
92.
Problems with Labor
Dystocia: Difficult labor that is prolonged or more painful
May occur because of problems caused by uterine contractions, fetus
presentation, or bone and tissues of maternal pelvis,
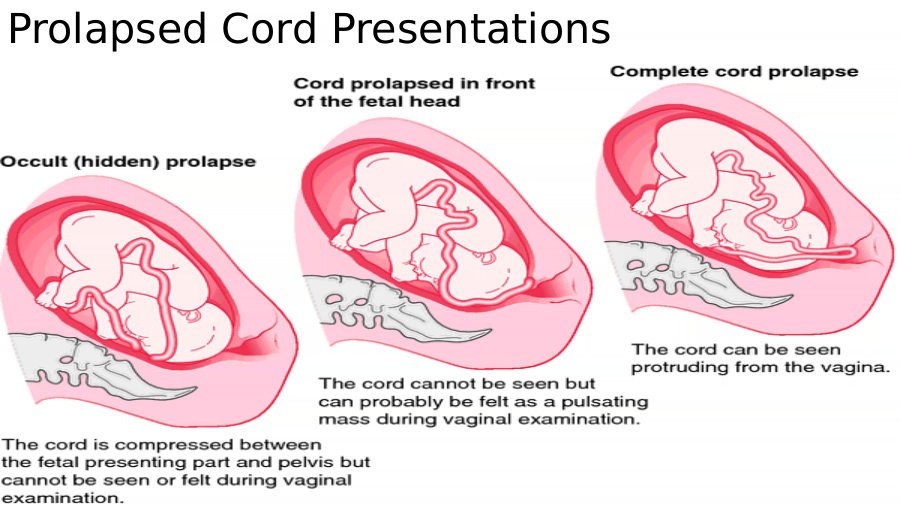
Prolapsed Cord: Umbilical cord displaced between presenting part and amnion or
protrudes through cervix, causing compression, compromising fetal circulation
Precipitous Labor and Delivery: Labor lasting less than 3 hours
Preterm Labor: Occurs after twentieth week, but before thirty seventh week of gestation
Contractions occur more frequently than every 10minutes, last 30 seconds or
longer, persist
93.
Problems with Labor
Premature Rupture of Membranes: Rupture of the amniotic sac before onset of true
labor, regardless of length of gestation
Rupture of Uterus: Complete or incomplete separation of uterine tissue as result of
tear in wall of uterus from stress of labor
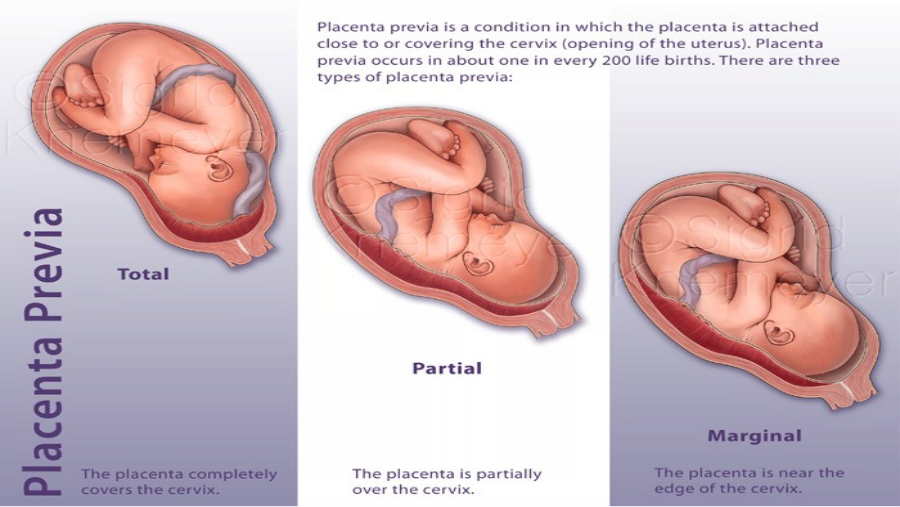
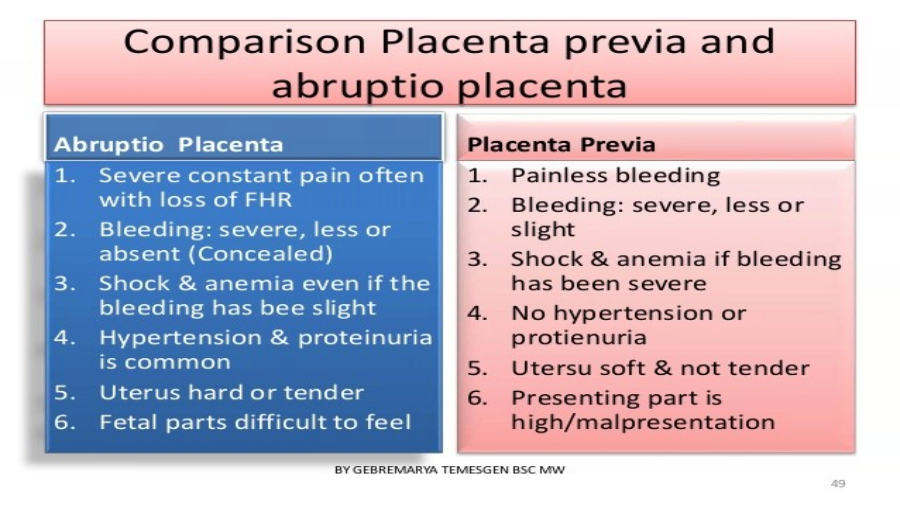
Placenta Previa: Improperly implanted placenta in the lower uterine segment, near
or over the internal cervical os
May be total, partial, marginal, or low-lying depending on how much of os is covered
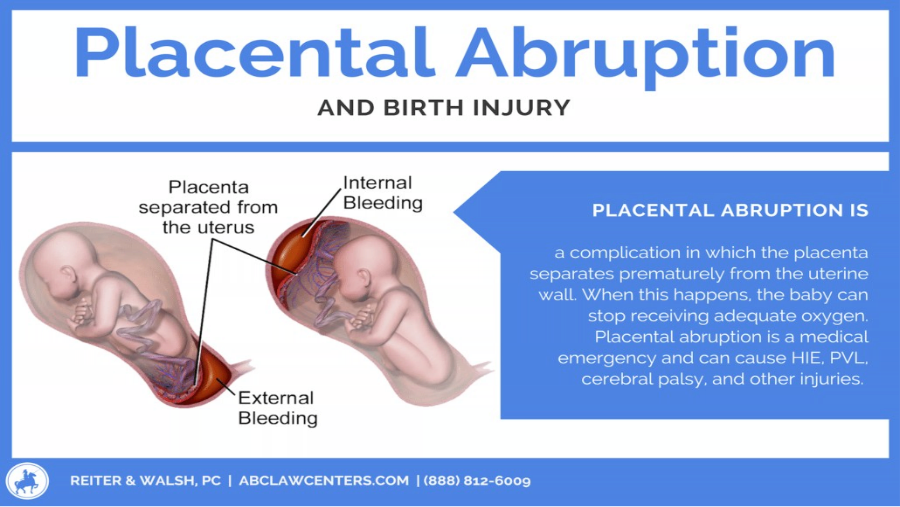
Abruptio Placentae: Premature separation of the placenta from the uterine wall after
twentieth week of gestation, before fetus is delivered
94.
Premature Rupture of Membranes: PROM
Rupture of the amniotic sac before onset of true labor,
regardless of length of gestation
Interventions
• Tests for gestational age
• Fluid pooling in vaginal area
• Vaginal examinations
• Positive Nitrazine and Fern Test
• Monitor for signs of infection
• Monitor maternal signs
• FHR
• Administer ABs
95.
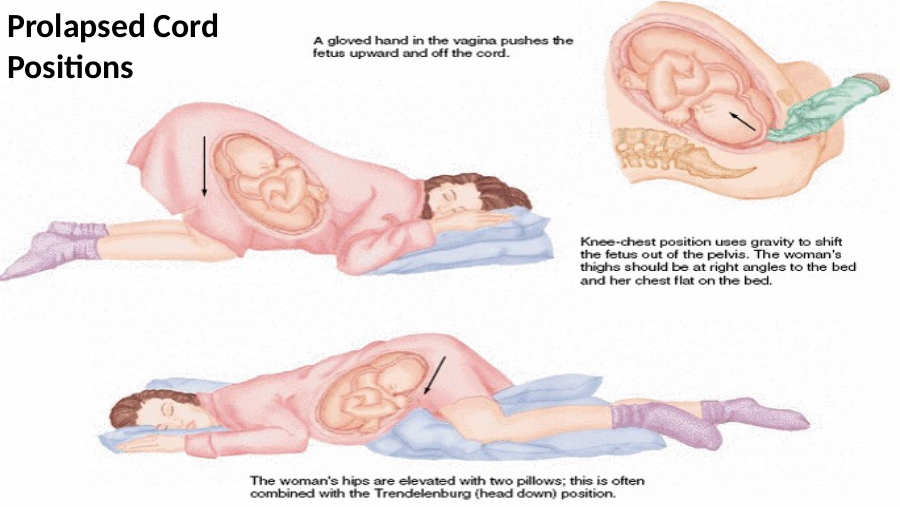
Prolapsed Cord Presentations
96.
Prolapsed Cord
Assessment Interventions
• Client may verbalize • Elevate the fetal presenting part that is lying
that something is on the cord by applying finger pressure with
coming through the a gloved hand
vagina • Extreme Trendelenburg/modified sim’s
• Umbilical Cord is position/Knee-chest position
visible or palpable • Oxygen: 8-10 L (Face Mask)
• FHR- Variable/Late • Monitor FHR & Fetal Hypoxia
• Violent fetal activity • IVF (Start or increase)
and then cease • Notify MD
• Prepare for immediate birth
99.
Placenta Previa
Assessment Interventions
• Sudden onset of • Monitor Ma- VS and FHR/Activity
painless, bright red • Ultrasound
vaginal
bleed(typically end • Vaginal examinations or any other
of pregnancy) examinations that may stimulate uterine
• Uterus/Fundus is activity are avoided (Contraindicated)
soft, relaxed, non- • Bed rest or side-lying position
tender • Monitor for bleeding (Shock)
• Fundal height higher • IVF/Tocolytics/Blood/Rhogam
than expected
101.
Abruptio Placentae
Assessment Interventions
• Dark Red Vaginal Bleeding • Ma- VS & FHR
• High placental abruption- No • Bed Rest, Oxygen- Face Mask
bleed
• Trendelenberg position
• Uterine pain/tender/Uterine
Rigidity • Prepare for surgery
• Severe Abdominal Pain • IVF/Tocolytics/Blood/ Rhogam
• Signs of fetal distress • Monitor for DIC
• Maternal Shock- depending on
the bleed
103.
Pre-term Labor: Labor before the 37 th
Assessment Interventions
• Contractions (pain or painless) • Stop the labor- identify the underlying
• Abdominal cramping- possible cause (Infections)
Diarrhea • Maintain bed rest or side lying position
• Lower back pain • Ma-VS & FHR
• Vaginal discharge- • IVF
thick/thin/clear/cloudy/bloody • Tocolytics
• Rupture of membranes
• Fibronectin
106.
Precipitous Delivery: Labor Lasting less
than 3 hours
Nursing Interventions:
• Be ready for the delivery & stay with client all the times
• Emotional Support
• Encourage to pant between contractions
• Do not prevent the fetus from being delievered
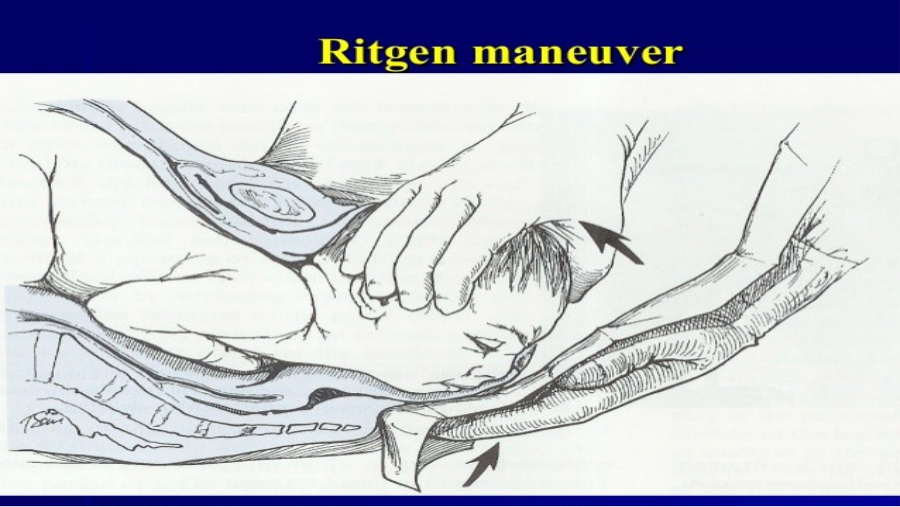
If delivery before the PROVIDER ARRIVAL-
• Apply gentle pressure to the fetal head upward toward the vagina to prevent
head injury (Ritgen Maneuver)
• Support fetal body
• Use gentle downward pressure to the anterior shoulder under the pubic symph.
108.
Amniotic Fluid Embolism
Assessment Interventions
• Sudden onset of ARDS • Call Rapid Response
• Sudden CP • Non-rebreather mask
• Cyanosis • Intubation/Ventilation
• Fetal Bradycardia • Left side lying position
• Emergency delivery: C-
section
• Emotional support
109.
Fetal Demise
Assessment Interventions
• Loss of fetal activity • Provide emotional support
• Absent FHR • Encourage patient and family to
• DIC verbalize their feelings
Low H & H • Religious and cultural beliefs
Prolonged PT & INR • IVF
Bleeding from puncture sites
• Blood products for DIC
110.
Rupture of the Uterus: Tear in the wall of
the Uterus
Assessment Interventions
• Severe abdominal pain/tenderness • Symptom mgx
• CP • Shock treatment
• Sudden stop of contractions • C-section
• Abdominal rigidity • Emotional support
• Absent FHR
• Ma-shock
• Fetal palpation outside the uterus
111.
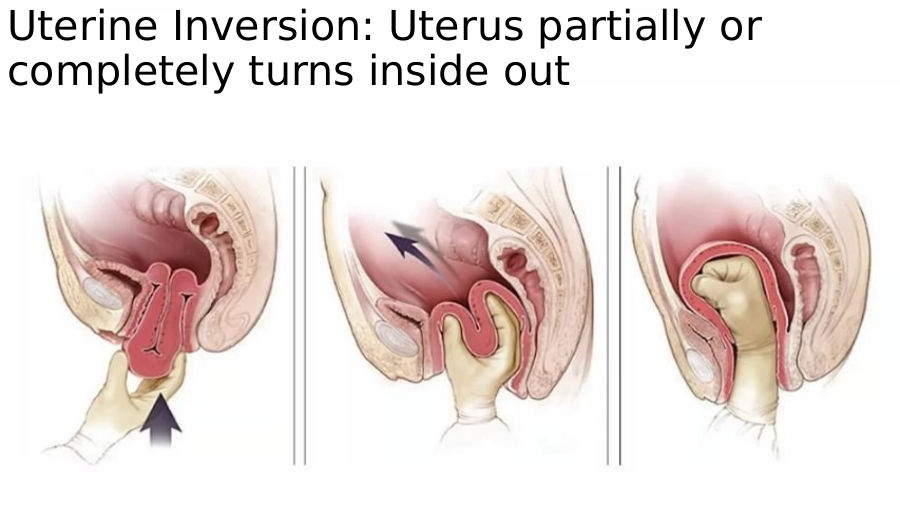
Uterine Inversion: Uterus partially or
completely turns inside out
112.
Uterine Inversion:
Assessment Intervention
• Depression in the fundal height • Shock mgx
• Uterus may be protruding through • Laparotomy
the vagina or visible at cervix
• Severe pain
• Bleeding- Shock
113.
Starts immediately after delivery; usually completed around week 6 following
Physiological Maternal Changes
• Involution: Rapid decrease in size of uterus as it returns to pre-pregnant state; fundal height
decreases one fingerbreadth (1 cm) per day
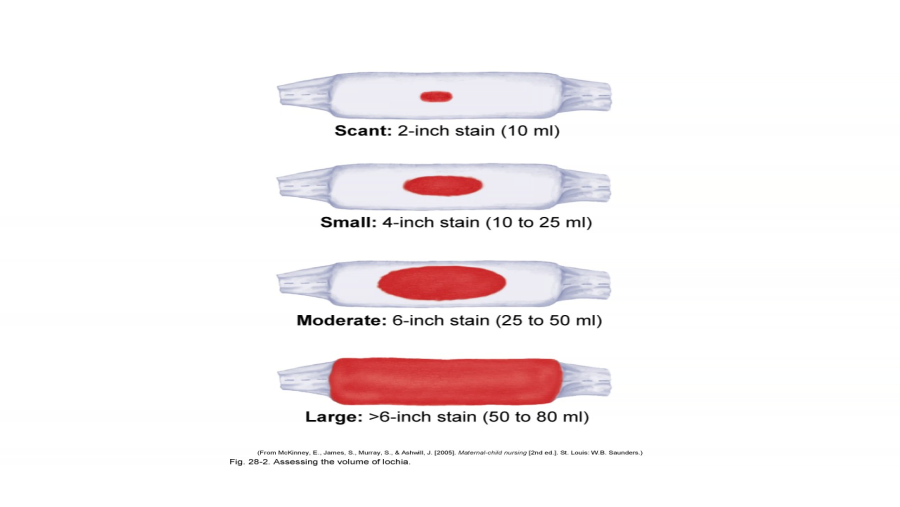
• Lochia: Discharge from uterus; consists of blood from vessels of placental site and debris
Rubra (red) occurs from delivery to day 3
Serosa (brownish-pink) occurs from days 4 to 10
Alba (white) occurs from days 10 to 14
• Cervix: Involution occurs; after 1 week, muscle begins to regenerate
• Vagina: Distention decreases, although muscle tone never completely restored to pregravida
state
114.
• Ovarian function and menstruation
• Menstrual flow resumes within 8 weeks in non–breast-feeding mothers, usually within 3 to 4
months in breast-feeding mothers
• Breasts
• Continue to secrete colostrum
• Become distended with milk on third day
• Engorgement occurs in 48 to 72 hours in non–breast-feeding mothers
• Breast-feeding will relieve engorgement
• Urinary tract
• May have initial urinary retention; diuresis begins in first
12 hours after delivery
• Gastrointestinal tract
• Mother usually hungry after delivery
• Constipation, hemorrhoids common
• Vital signs
• Hyperthermia common in first 24 hours ( T may rise to 100.4)
• Bradycardia common in first week ( may fall to 50, greater than 100, may indicate excessive blood
loss)
• BP should be normal, if may be hypovolemia, if check preeclampsia
115.
Postpartum Interventions
• Administer Rho(D) immune globulin (RhoGAM) as prescribed within
72 hours postpartum to Rh-negative mother who has given birth to
Rh-positive baby.
• Monitor maternal vital signs, lochia, fundal height, perineal edema
and discoloration, presence of signs of hemorrhage, breasts for
engorgement, bowel status, intake and output
• Facilitate bonding with newborn
• Client teaching
• Demonstrate newborn care skills as appropriate
• Demonstrate breast-feeding or formula-feeding techniques
• Kegel exercises
• Diet
117.
Postpartum Discomforts
– Afterbirth pains: Occur as result of contractions of uterus; more common in multiparas, breast-feeding
mothers, clients treated with oxytocin (Pitocin)
• Educate the client as to the cause of the afterbirth pains
– Perineal discomfort: Occurs as result of delivery
• Apply ice packs to perineum during first 24 hours
• After first 24 hours, apply warmth via sitz bath
– Episiotomy: Incision made into perineum to enlarge vaginal outlet and facilitate delivery
• Educate client to perform perineal care after voiding
• Encourage use of analgesic spray, analgesics PO as prescribed
– Perineal lacerations: May occur as result of tear of vaginal outlet during delivery
• Interventions as for perineal discomfort from episiotomy as prescribed
– Breast discomfort: Occurs as result of engorgement
• Wear supportive bra at all times
• Encourage use of ice packs between feedings if breast-feeding
– Constipation: Occurs as result of edema and pain following delivery
• Administer stool softeners as prescribed
• Encourage fluid intake
– Postpartum blues: Occurs as result of physiological and emotional stress
• Encourage verbalization of feelings, concerns
118.
Post Partum Complications
Cystitis: Infection of bladder
Hematoma: Localized collection of blood into tissues of reproductive tract after delivery
Hemorrhage: Bleeding of 500 mL or more following delivery ( high cause of maternal morbidity)
Infection: Any infectious process of reproductive organs that occurs within 28 days of delivery or
abortion
Mastitis: Inflammation of breast as result of infection, usually occurring in breast-feeding mothers, 2 to
3 weeks after delivery
Pulmonary Embolism: Passage of thrombus, often originating in one uterine or other pelvic vein, into
lungs, where it disrupts circulation of blood
Thrombophlebitis: Condition in which clot forms in vessel wall as result of inflammation of vessel wall
119.
Nursing Interventions
Mastitis Postpartum Blues/Emotional Needs
1. Wear supportive bra/sports bra at all 1. Emotional support
times- even sleeping 2. Encourage to verbalize feelings
2. Use ice-packs between feedings 3. Engage family and spousal in the
3. Use warm soaks or warm showers discussion of child care
before feeding 4. Educate family members about the
4. Use cabbage leaves growth & development appropriate
for the age
5. All clients are screened for
depression during pregnancy and
postpartum period.
120.
• Put baby to breast as soon as mother and baby in stable condition
• Remain with mother during feeding until she feels secure with baby and
procedure
• Assess LATCH
Latch achieved by infant
Audible swallowing
Type of nipple
Comfort of mother
Help given to mother during nursing
• Educate mother that uterine cramping may occur while nursing, breasts may leak
between feedings
• Educate about general hygiene and washing breasts once daily with water
• Educate about increasing caloric intake
200 to 500 cal/day as well as increasing fluid intake
121.
Breast feeding procedure
1. Wash hands and assume a comfortable position
2. Start the feeding with which the last feeding ended
3. Brush the newborn’s lower lip with the nipple
4. Tick the lips to have the newborn open the mouth wide
5. Guide the nipple and surrounding areola into the mouth
6. Encourage the newborn to nurse on each breast for at least 15-20 minutes
7. After the nursing, release suction by depressing the newborn’s chin or inserting
a clean finger into the newborn’s mouth
8. Burp the newborn after the first breast
9. Repeat the steps with the second breast and burp the newborn again
10. Listen for audible sucking and swallowing
122.
Initial Care of the Newborn
• Monitor for nasal flaring, grunting, retractions, abdominal respirations
• Monitor vital signs, signs of hypothermia or hyperthermia
• Suction mouth and nares
• Dry newborn
• Stimulate crying
• Maintain temperature stability
• Keep newborn with mother to facilitate bonding
• Position newborn on side or abdomen or in modified Trendelenburg’s position
• Ensure newborn’s proper identification
• Footprint newborn and fingerprint mother as per agency policy
• Place matching bracelets on mother and newborn
126.
Initial Care of the Newborn
Apgar scoring system
Apgar score at 1 minute and 5 minutes, scoring from 0 (very poor) to 2
(excellent) in following areas as heart rate, respiratory rate, muscle tone,
reflex irritability, skin color
Apgar scoring interventions
8 to 10: No intervention required except to support infant’s spontaneous
efforts
4 to 7: Gently stimulate; rub infant’s back; administer oxygen to infant
0 to 3: Infant requires resuscitation
127.
Initial Care of the Newborn
General guidelines
• Keep neonate warm; complete examination from general to specific
• Vital signs: Heart rate and respirations should be calculated based on 1-minute assessment
Body measurements
• Length: 45 to 55 cm
• Weight: 2500 to 4300 g
• Head circumference: 33 to 35.5 cm
• Chest circumference: 30 to 33 cm
Cardiovascular system
• 1-minute apical pulse, especially assessing for murmurs , auscultate for one full
minute at the PMI
• Normal heart rate, 120 to 160 beats/min
128.
Initial Care of the Newborn
Respiratory system
• Normal respiration rate, 30 to 60 breaths/min, count for one full minute
• Signs of respiratory distress, including nasal flaring, grunting, cyanosis,
bradycardia, apnea
Thermal regulatory system
• Normal temperature, 97.7° to 99.5° F axillary
• Does not shiver to produce heat
• Keep infant in neutral thermal environment (NTE)
• Take temperature every hour for first four hours of life, then every 4
hours for rest of 24-hour period
129.
Initial Care of the Newborn
• Head to toe assessment
• Neuromuscular assessment- absence of expected reflexes may indicate a
problem
• Gestational age assessment- Ballard scale
Neuromuscular Criteria Physical Criteria
Posture Skin
Square window Ear/eye
Arm recoil Lanugo hair
Popliteal angle Plantar surface
Scarf sign Breast bud
Heel To ear Genitals
130.
• https://www.youtube.com/watch?v=vdiCep6OStA
• Sucking and rooting: Touch newborn’s lip, cheek, or corner of mouth with nipple;
newborn will turn head toward nipple
• Swallowing: Occurs spontaneously after sucking, obtaining fluids
• Tonic neck or fencing: Turn head to one side while newborn is falling asleep; when facing
left, left arm and leg extend and right arm and leg flex; vice versa if head is turned to
right
• Palmar-plantar grasp: Place finger in palm of newborn’s hand, then place finger at base
of toes; newborn’s fingers curl around examiner’s fingers, toes curl downward
131.
• Moro: Hold newborn in semisitting position, allow head and trunk to fall backward
to at least 30° angle; newborn will symmetrically abduct and extend arms
• Startle: Examiner makes loud noise; newborn’s arms adduct while elbows flex
• Pull-to-sit: Pull newborn up from wrist while in supine position; head will lag until
newborn is in upright position, then will level with chest, then fall forward
• Babinski: Gently stroke upward along lateral aspect of sole and then along ball of
foot; newborn’s toes will hyperextend with big toe dorsiflexing; after 1 year of age,
indicates neurological deficit
• Crawling: Place newborn on abdomen; newborn will begin to make crawling
movements with arms and legs
132.
Newborn Safety
Infant identification
• Footprint newborn, fingerprint mother
• Identification bands placed on mother, infant, father, other support
person(s) at birth
• Information on each band includes number that identifies mother and
baby
Infant abduction
• Nurse’s role is protection of newborn from abduction
• Maintain security measures (e.g., locked units) as per agency policy
• Check visitors for identification as per agency policy
• If locked door alarm goes off, respond quickly as per agency policy
133.
Preterm Newborn: Primary concern is immaturity of all body systems
• Respirations irregular, with periods of apnea
• Body temperature below normal
• Poor suck and swallow reflexes
• Diminished bowel sounds
• Thin extremities, with minimal creasing on soles and palms
• No maintenance of flexion in extremities
• Lanugo present in wooly patches
• Thin skin, with visible blood vessels and minimal subcutaneous fat pads; skin may appear jaundiced
• Undescended testes in boys, narrow labia in girls
• Monitor vital signs every 2 to 4 hours
• Maintain cardiopulmonary function; administer oxygen as prescribed
• Monitor intake, output, electrolyte balance, daily weight
• Maintain neutral thermal environment
• Handle newborn carefully, changing position every 1 to 2 hours
• Avoid exposure to infections
134.
Post-term Newborn: Neonate born after 42 weeks’ gestation
Hypoglycemia; parchment-like skin without lanugo; long fingernails, extended over
fingers; profuse scalp hair; long, thin body; wasting of fat and muscle in extremities;
meconium staining on nails and umbilical cord
• Provide normal newborn care
• Monitor for meconium aspiration
• Monitor for hypoglycemia
• Maintain newborn’s temperature
Small for Gestational Age: Neonate plotted at or below tenth percentile on intrauterine
growth curve
Large for Gestational Age: Neonate plotted at or above the ninetieth percentile on
intrauterine growth curve
135.
Newborn Complications
• RDS Respiratory Distress Syndrome
• BPD Bronchopulmonary Dysplasia
• MAS Meconium Aspiration Syndrome
• TTN Transient Tachypnea of the Newborn
• IVH Intraventricular Hemorrhage
• ROP Retinopathy of Prematurity
• NEC Necrotizing Enterocolitis
• Hyperbilirubinemia
• Sepsis
• TORCH
• IDM Infant of Diabetic Mom
136.
Mom Baby
• Lung Surfactants
• Oxytocin (Pitocin)
• Eye Prophylaxis for the Neonate
• Medications Used to Manage
Postpartum Hemorrhage • Vitamin K (AquaMEPHYTON)
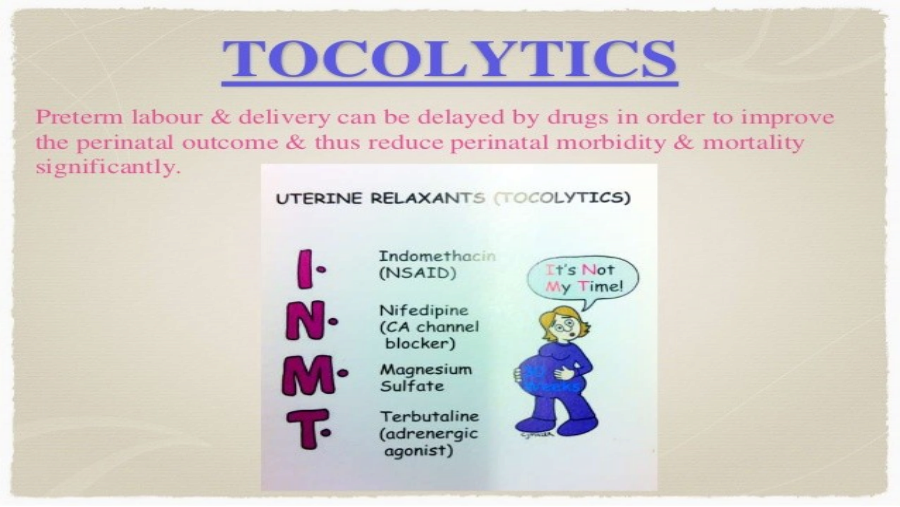
• Tocolytics • Hepatitis B Vaccine (HBV)
• Prostaglandins
• Magnesium Sulfate
• Opioid Analgesics
• Betamethasone
• Rho(D) Immune Globulin
• Rubella Vaccine